Introduction: The Anterior Lateral thigh flap (ALT) free flap can be considered one of the reconstructive tools in lower leg and foot reconstruction. It has a long and reliable pedicle, and dissection is comparatively easy, which makes it extremely suitable as a free flap. This study aimed to evaluate the versatility of the flap in covering lower leg and foot defects. Methods: This was a prospective observational study conducted in the Department of Plastic Surgery, Rangpur Medical College Hospital, Rangpur, Bangladesh, from January 2023 to December 2023. In our study, we included 16 patients with defects in the lower leg and foot who received an ALT-free flap as a reconstructive treatment. We analyzed the preoperative, intraoperative, and postoperative variables of our respondents. Results: In this study, 16 patients (12 males and 4 females) with an average of 34.25 years old were included. Among them 13 were traumatic cases, 2 electrical burn wounds, and one oncologic case. Survival rates of the free flap were 87.5% (14) with two failure cases. There were no complications at the donor site. In this study, 75% (12) cases showed excellent outcomes where there were no signs, or symptoms of venous congestion or arterial insufficiency, no infection or dehiscence, and the donor site was primarily closed with good flap adhesion. Conclusion: This study shows that the ALT-free flap is a versatile flap that allows it to cover the defect successfully and ALT adaptation was satisfactory in terms of varied location and size.
| Published in | American Journal of Health Research (Volume 12, Issue 6) |
| DOI | 10.11648/j.ajhr.20241206.17 |
| Page(s) | 230-236 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Anterolateral Thigh Flap, Split Thickness Skin Graft, Versatility, Foot Reconstruction
Demographic variables | N | P (%) |
|---|---|---|
Age | ||
< 20 years | 2 | 12.5 |
20-29 years | 5 | 31.25 |
30-39 years | 3 | 18.75 |
>39 years | 6 | 37.5 |
Mean ±SD (years) | 34.25 ±15.27 | |
Gender | ||
Male | 12 | 75 |
Female | 4 | 25 |
Smoking status | ||
Yes | 6 | 37.5 |
No | 10 | 62.5 |
Defect origin | ||
Trauma | 13 | 81.25 |
Marjolin ulcer | 1 | 6.25 |
Electric burn | 2 | 12.5 |
Location of defect | ||
Sole & Heel (left/right) | 5 | 31.25 |
Dorsum of foot (left /right) | 4 | 25 |
The middle part of leg | 1 | 6.25 |
Lower 1/3rd of rt leg | 6 | 37.5 |
Mean Size (length, cm) | 6.625 ±1.902 | |
Mean Size (wide, cm) | 3.868 ± 0.994 | |
Mean Time delay (days) | 17.125 ± 5.760 | |
Co-morbidities | ||
DM | 3 | 18.75 |
Hypothyroidism | 1 | 6.25 |
Intraoperative variables | N | P (%) |
|---|---|---|
Type of flap | ||
Fascio cutaneous | 12 | 75.0 |
Fat cutaneous | 4 | 25.0 |
Number of perforating arteries | ||
1 | 13 | 81.3 |
2 | 3 | 19.7 |
Type of perforating arteries | ||
Septal | 4 | 25.0 |
Muscular | 12 | 75.0 |
Recipient vascular bundle | ||
Posterior tibial vessels | 4 | 25.0 |
Anterior tibial vessels | 12 | 75.0 |
Stitches | ||
8/o prolene | 16 | 100.0 |
Arterial anastomosis | ||
End to end | 14 | 87.5 |
End to side | 2 | 12.5 |
Venous anastomosis | ||
End to end | 16 | 100.0 |
Donor site closure | ||
Primary | 12 | 75.0 |
STSG | 4 | 25.0 |
Result | Flap survival rate | Donor site |
|---|---|---|
Excellent | Flap completely survived No venous congestion or arterial insufficiency, no infection, and excellent flap adhesion. | No infection, no wound dehiscence, closed primarily. |
Satisfactory | Flap survives with few complications. | Mild infection, Wound dehiscence, secondary closure |
Poor | Flap failure or loss, severe complications | Primary, Secondary closure, or STSG |
Outcome | N | P (%) |
|---|---|---|
Excellent | 12 | 75 |
Satisfactory | 2 | 12.5 |
Poor | 2 | 12.5 |
ALT | Anterior Lateral Thigh Flap |
VL | Vastus Lateralis |
STSG | Split-Thickness Skin Graft |
COPD | Chronic Obstructive Pulmonary Disease |
| [1] | Song Yg, Chen Gz, Song Yl. The Free Thigh Flap: A New Free Flap Based On The Septocutaneous Artery. Br J Plast Surg 1984; 37: 149–159. |
| [2] | Mardini S, Lin Ch, Wei Fc. In: Blondeel Pn, Morris Sf, Hallock Gg, Et Al, Eds. Perforator Flaps: Anatomy, Technique & Clinical Applications. St. Louis, Mo: Quality Medical Publishing; 2006: 617–633. |
| [3] | Nosrati N, Chao Ah, Chang Dw, Yu P. Lower Extremity Reconstruction With The Anterolateral Thigh Flap. Journal Of Reconstructive Microsurgery. 2012 May; 28(04): 227-34. |
| [4] | Lee N, Roh S, Yang K, Kim J. Reconstruction Of Hand And Forearm After Sarcoma Resection Using Anterolateral Thigh Free Flap. J Plast Reconstr Aesthet Surg 2009; 62(12): E584–E586. |
| [5] | Gravvanis A, Tsoutsos D, Karakitsos D, Iconomou T, Papadopoulos O. Blood Perfusion Of The Free Anterolateral Thigh Perforator Flap: Its Beneficial Effect In The Reconstruction Of Infected Wounds In The Lower Extremity. World J Surg 2007; 31(1): 11–18. |
| [6] | Kuo Yr, Kuo Mh, Chou Wc, Liu Yt, Lutz Bs, Jeng Sf. One-Stage Reconstruction Of Soft Tissue And Achilles Tendon Defects Using A Composite Free Anterolateral Thigh Flap With Vascularized Fascia Lata: Clinical Experience And Functional Assessment. Ann Plast Surg 2003; 50(2): 149–155. |
| [7] | Heller L, Kronowitz Sj. Lower Extremity Reconstruction. J Surg Oncol 2006; 94(6): 479–489. |
| [8] | Park Je, Rodriguez Ed, Bluebond-Langer R, Et Al. The Anterolateral Thigh Flap Is Highly Effective For Reconstruction Of Complex Lower Extremity Trauma. J Trauma 2007; 62(1): 162–165. |
| [9] | Demirtas Y, Neimetzade T, Kelahmetoglu O, Guneren E. Comparison Of Free Muscle And Perforator Skin Flaps For Soft Tissue Reconstruction Of The Foot And Ankle. Foot Ankle Int 2010; 31(1): 53–58.. |
| [10] | Hong Jp, Kim Ek. Sole Reconstruction Using Anterolateral Thigh Perforator Free Flaps. Plast Reconstr Surg 2007; 119(1): 186–193. |
| [11] | Ng Rw, Chan Jy, Mok V, Li Gk. Clinical Use Of A Pedicled Anterolateral Thigh Flap. J Plast Reconstr Aesthet Surg 2008; 61(2): 158– 164. |
| [12] | Friji Mt, Suri Mp, Shankhdhar Vk, Ahmad Qg, Yadav Ps. Pedicled Anterolateral Thigh Flap: A Versatile Flap For Difficult Regional Soft Tissue Reconstruction. Ann Plast Surg 2010; 64(4): 458–461. |
| [13] | Gravvanis Ai, Tsoutsos Da, Karakitsos D, Et Al. Application Of The Pedicled Anterolateral Thigh Flap To Defects From The Pelvis To The Knee. Microsurgery 2006; 26(6): 432–438. |
| [14] | Wei Fc, Jain V, Celik N, Chen Hc, Chuang Dc, Lin Ch. Have We Found An Ideal Soft-Tissue Flap? An Experience With 672 Anterolateral Thigh Flaps. Plastic And Reconstructive Surgery. 2002 Jun 1; 109(7): 2219-26. |
| [15] | Biswas D, Kalam Ma, Ahmed T, Khan Mrk. Results Of Microvascular Free Flap For Reconstruction Of Soft Tissue Defects: Our Early Experience. Bdjps 2012; 3(2): 33-37. |
| [16] | Michael R. Christy, Avron Lipschitz, Eduardo Rodriguez, Karan Chopra, Nance Yuan, Early Postoperative Outcomes Associated With The Anterolateral Thigh Flap In Gustiloiiib Fractures Of The Lower Extremity. Ann Plast Surg2014; 72: 80-83. |
| [17] | Hossein Nasajpour, Matthew H. Steele, Anterolateral Thighfree Flap For “Head-To-Toe” Reconstruction. Ann Plast Surg 2011; 66: 530–533. |
| [18] | Nerlich AG, Zink A, Szeimies U, Hagedorn HG. Ancient Egyptian prosthesis of the big toe. The Lancet. 2000 Dec 23; 356(9248): 2176-9. |
| [19] | Park Je, Rodriguez Ed, Bluebond-Langer R, Et Al. The Anterolateral Thigh Flap Is Highly Effective For Reconstruction Of Complex Lower Extremity Trauma. J Trauma. 2007; 62: 162-165. |
| [20] | Jeng Sf, Wei Fc. Classification And Reconstructive Options In Foot Plantar Skin Avulsion Injuries. Plast Reconstr Surg 1997; 99: 1695-1705. |
| [21] | Kohli Js, Pande S, Bajaja Sp. Large Transversefasciocutaneous Leg Flap: Whole Leg Flap In Prosess Citation. Br J Plast Surg 2000; 53: 495-8. |
| [22] | Rahim S. Nazerali, Lee L. Q. Pu. Free Tissue Transfer To Thelower Extrimity A Paradigm Shift In Flap Selection For Soft Tissue Reconstruction Ann Plast Surg 2013; 70: 419-422. |
| [23] | Serafin D, Georgiade Ng, Smith Dh. Comparison Of Freeflaps With Pedicled Flaps For Coverage Of Defects Of The Leg Or Foot. Plast Reconstr Surg 2007; 59: 492-9. |
| [24] | Gedebou Tm, Wei Fc, Lin Ch. Clinical Experience Of 1284 Free Anterolateral Thigh Flaps. Handchir Mikrochir Plast Chir 2002; 34(4): 239-44. |
| [25] | Mureau Ma, Posch Na, Meeuwis Ca, Hofer So. Anterolateral Thigh Flap Reconstruction Of Large External Facial Skin Defects: A Follow-Up Study On Functional And Aesthetic Recipient- And Donor-Site Outcome. Plast Reconstr Surg 2005; 115(4): 1077-86. |
| [26] | Colterjohn Nr, Davis Am, O'sullivan B, Catton Cn, Wunder Js, Bell Rs. Functional Outcome In Limb-Salvage Surgery For Soft Tissue Tumours Of The Foot And Ankle. Sarcoma 1997; 1(2): 67–74. |
| [27] | Yu P. Characteristics Of The Anterolateral Thigh Flap In A Western Population And Its Application In Head And Neck Reconstruction. Head Neck 2004; 26(9): 759–769. |
APA Style
Hamid, M. A., Sultana, S. N., Mukit, S. M. A., Biswas, G. (2024). The Anterolateral Thigh Flap for Lower Leg & Foot Reconstruction in a Tertiary Hospital in Northern Bangladesh: Our Observation and Outcome. American Journal of Health Research, 12(6), 230-236. https://doi.org/10.11648/j.ajhr.20241206.17
ACS Style
Hamid, M. A.; Sultana, S. N.; Mukit, S. M. A.; Biswas, G. The Anterolateral Thigh Flap for Lower Leg & Foot Reconstruction in a Tertiary Hospital in Northern Bangladesh: Our Observation and Outcome. Am. J. Health Res. 2024, 12(6), 230-236. doi: 10.11648/j.ajhr.20241206.17
AMA Style
Hamid MA, Sultana SN, Mukit SMA, Biswas G. The Anterolateral Thigh Flap for Lower Leg & Foot Reconstruction in a Tertiary Hospital in Northern Bangladesh: Our Observation and Outcome. Am J Health Res. 2024;12(6):230-236. doi: 10.11648/j.ajhr.20241206.17
@article{10.11648/j.ajhr.20241206.17,
author = {M. A. Hamid and Sayeda Niger Sultana and Shah Md. Al Mukit and Goutam Biswas},
title = {The Anterolateral Thigh Flap for Lower Leg & Foot Reconstruction in a Tertiary Hospital in Northern Bangladesh: Our Observation and Outcome
},
journal = {American Journal of Health Research},
volume = {12},
number = {6},
pages = {230-236},
doi = {10.11648/j.ajhr.20241206.17},
url = {https://doi.org/10.11648/j.ajhr.20241206.17},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajhr.20241206.17},
abstract = {Introduction: The Anterior Lateral thigh flap (ALT) free flap can be considered one of the reconstructive tools in lower leg and foot reconstruction. It has a long and reliable pedicle, and dissection is comparatively easy, which makes it extremely suitable as a free flap. This study aimed to evaluate the versatility of the flap in covering lower leg and foot defects. Methods: This was a prospective observational study conducted in the Department of Plastic Surgery, Rangpur Medical College Hospital, Rangpur, Bangladesh, from January 2023 to December 2023. In our study, we included 16 patients with defects in the lower leg and foot who received an ALT-free flap as a reconstructive treatment. We analyzed the preoperative, intraoperative, and postoperative variables of our respondents. Results: In this study, 16 patients (12 males and 4 females) with an average of 34.25 years old were included. Among them 13 were traumatic cases, 2 electrical burn wounds, and one oncologic case. Survival rates of the free flap were 87.5% (14) with two failure cases. There were no complications at the donor site. In this study, 75% (12) cases showed excellent outcomes where there were no signs, or symptoms of venous congestion or arterial insufficiency, no infection or dehiscence, and the donor site was primarily closed with good flap adhesion. Conclusion: This study shows that the ALT-free flap is a versatile flap that allows it to cover the defect successfully and ALT adaptation was satisfactory in terms of varied location and size.
},
year = {2024}
}
TY - JOUR T1 - The Anterolateral Thigh Flap for Lower Leg & Foot Reconstruction in a Tertiary Hospital in Northern Bangladesh: Our Observation and Outcome AU - M. A. Hamid AU - Sayeda Niger Sultana AU - Shah Md. Al Mukit AU - Goutam Biswas Y1 - 2024/11/29 PY - 2024 N1 - https://doi.org/10.11648/j.ajhr.20241206.17 DO - 10.11648/j.ajhr.20241206.17 T2 - American Journal of Health Research JF - American Journal of Health Research JO - American Journal of Health Research SP - 230 EP - 236 PB - Science Publishing Group SN - 2330-8796 UR - https://doi.org/10.11648/j.ajhr.20241206.17 AB - Introduction: The Anterior Lateral thigh flap (ALT) free flap can be considered one of the reconstructive tools in lower leg and foot reconstruction. It has a long and reliable pedicle, and dissection is comparatively easy, which makes it extremely suitable as a free flap. This study aimed to evaluate the versatility of the flap in covering lower leg and foot defects. Methods: This was a prospective observational study conducted in the Department of Plastic Surgery, Rangpur Medical College Hospital, Rangpur, Bangladesh, from January 2023 to December 2023. In our study, we included 16 patients with defects in the lower leg and foot who received an ALT-free flap as a reconstructive treatment. We analyzed the preoperative, intraoperative, and postoperative variables of our respondents. Results: In this study, 16 patients (12 males and 4 females) with an average of 34.25 years old were included. Among them 13 were traumatic cases, 2 electrical burn wounds, and one oncologic case. Survival rates of the free flap were 87.5% (14) with two failure cases. There were no complications at the donor site. In this study, 75% (12) cases showed excellent outcomes where there were no signs, or symptoms of venous congestion or arterial insufficiency, no infection or dehiscence, and the donor site was primarily closed with good flap adhesion. Conclusion: This study shows that the ALT-free flap is a versatile flap that allows it to cover the defect successfully and ALT adaptation was satisfactory in terms of varied location and size. VL - 12 IS - 6 ER -
Department of Plastic Surgery, Rangpur Medical College Hospital, Rangpur, Bangladesh
Department of Gynaecology and Obstetrics, Prime Medical College Hospital, Rangpur, Bangladesh
Department of Plastic Surgery, Rangpur Medical College Hospital, Rangpur, Bangladesh
Department of Anaesthesia, Rangpur Medical College Hospital, Rangpur, Bangladesh
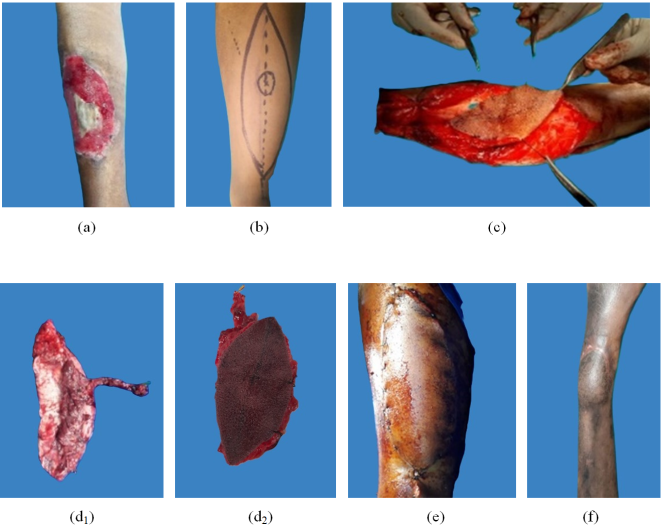
Figure 1. (a): Post-traumatic defect in the lower leg; 1 (b): Design of ALT flap; 1(c): Elevation of the flap; 1(d1 &d2): After harvesting of flap; 1(e): After inset of flap;; 1(f): After 1 year picture.
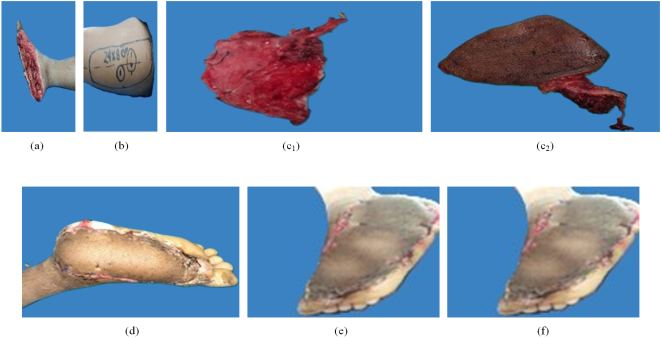
Figure 2. (a): Post-traumatic defect in the sole; 2 (b): Designing of ALT flap 2(c1 & c2): After harvest of flap; 2(d): At 8th POD View; 2(e): At 14th POD; 2(f): After 6months picture.

Figure 3. (a): Preoperative picture of the defect in the dorsum of the foot; (b): Post-operative picture.
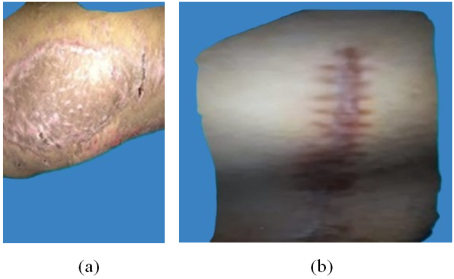
Figure 4. Donor site.
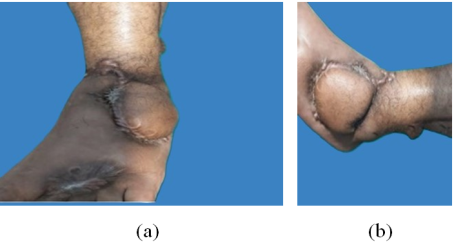
Figure 5. After 1-year follow-up picture.
Information

