Abstract
Background: Helicobacter pylori infection has been reported to affect more than half of the global population. The persistence of H. pylori infection results to chronic gastritis and peptic ulcer disease. Despite this burden there is limited published studies regarding proportion of Helicobacter pylori infected children that require treatment in many settings in low and middle-income countries (LMICs). Therefore this study aimed to determine the epidemiology of and factors associated with Helicobacter pylori infection and proportion requiring treatment among symptomatic children in northwestern Tanzania. Methodology: This was a hospital based cross-sectional study conducted at BMC hospital in Northwestern Tanzania from December 2021 and April 2022 among outpatient children aged 1 to 15 years with gastrointestinal symptoms. The main study outcome (event) was presence of H. pylori infection as evidence by positive stool antigen test. Independent factors associated with H. pylori infection were determined by logistic regression model. The significance level was set at p-value of <0.05. Oesophagogastroduodenoscopy (OGD) was performed to the randomly serially selected representative sample of symptomatic children with positive H. pylori stool antigen test to determine the proportion of children requiring treatment. Results: A total of 422 symptomatic children were included in the study. The median age was 7 [IQR 3 – 10] years. The prevalence of H. pylori infection was 105 (24.9%). More than half of the participants (56.4%) were males. The risk of H. pylori infection was significantly associated with increase in age (OR= 1.09; 95%CI; 1.03 – 1.15; P= 0.002), and abdominal pain (OR=2.2; 95%CI 1.2 – 4.0; P= 0.01). About 55 participants were randomly selected for OGD among 100 children above or equal 2 years of age with positive stool antigen for H. pylori. The majority were found to have lesion warranting treatment. These lesions included gastritis 47 (85.5%), duodenal ulcers 2 (3.6%) and gastric ulcers 1 (1.8%). Conclusion: About a quarter of the enrolled children had H. pylori infection. Increase in age and abdominal pain were independently associated with H. pylori infection. Most H. pylori stool antigen test positive children had endoscopic lesions that warranted treatment. Therefore every H. pylori stool antigen test positive child needs eradication therapy.
|
Published in
|
American Journal of Pediatrics (Volume 10, Issue 2)
|
|
DOI
|
10.11648/j.ajp.20241002.12
|
|
Page(s)
|
52-62 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2024. Published by Science Publishing Group
|
Keywords
Prevalence, Factors, Helicobacter Pylori Infection, Treatment, Symptomatic Children, Tanzania
1. Introduction
Helicobacter pylori (
H. pylori) infection have been reported to be the most common human infection, affecting about 50% of the global population
| [1] | Aitila P, Mutyaba M, Okeny S, Ndawula Kasule M, Kasule R, Ssedyabane F, et al. Prevalence and Risk Factors of Helicobacter pylori Infection among Children Aged 1 to 15 Years at Holy Innocents Children’s Hospital, Mbarara, South Western Uganda. J Trop Med. 2019; 93(3): 1–7. eCollection 2019. https://doi.org/10.1155/2019/9303072 |
| [2] | Hooi JKY, Lai WY, Ng WK, Suen MMY, Underwood FE, Tanyingoh D, et al. Global Prevalence of Helicobacter pylori Infection: Systematic Review and Meta-Analysis. Gastroenterology. 2017; 153(2): 420-429. https://doi.org/10.1053/j.gastro.2017.04.022 |
| [3] | Salih BA. Helicobacter pylori Infection in Developing Countries : The Burden for How Long ? Saudi J Gastroenterol. 2009; 15(3): 201–207. https://doi.org/10.4103/1319-3767.54743 |
[1-3]
. By the age of 5 years about 50% of children are infected and this rate has been reported to exceed 90% during adulthood
| [4] | Bardhan PK. Epidemiological features of Helicobacter pylori infection in developing countries. Clin Infect Dis. 1997; 25(5): 973–8. https://doi.org/10.1086/516067 |
[4]
. A recently hospital based study in Uganda among children aged 1 to 15 years found the prevalence to be 24.3% and this increased with increasing age
| [1] | Aitila P, Mutyaba M, Okeny S, Ndawula Kasule M, Kasule R, Ssedyabane F, et al. Prevalence and Risk Factors of Helicobacter pylori Infection among Children Aged 1 to 15 Years at Holy Innocents Children’s Hospital, Mbarara, South Western Uganda. J Trop Med. 2019; 93(3): 1–7. eCollection 2019. https://doi.org/10.1155/2019/9303072 |
[1]
. A previous study which was conducted in the Bugando Medical Center on
Helicobacter pylori infection in children < 12 years of age reported a prevalence of 42.9%. It was clearly reported that the prevalence increased with increase in age
| [5] | Jaka H et al. Prevalence and risk factors associated with Helicobacter pylori infections in Tanzanian children. Catholic University of Health and Allied Sciences. 2016. |
[5]
. Treating all children could expose them to unnecessary antibiotics therapy hence promoting antimicrobial resistance (AMR) development. On the other hand invasive tests to establish causes of symptoms are not widely available in many settings in LMICs. The joint ESPGHAN/NASPGHAN guidelines recommend confirmation of
H. pylori infection by invasive methods such as upper gastrointestinal endoscopy, thereafter provision of eradication therapy preferably proton pump inhibitor plus two antibiotics for 14 days to the
H.
pylori infected children who have gastric or duodenal ulceration or erosions. Confirmation of eradication is performed at least 4 weeks after completion of antibiotic treatment and 2 weeks after proton pump inhibitors (PPI) cessation using the urea breath test or
H. pylori stool antigen test
| [6] | Jones NL, Koletzko S, Goodman K, Bontems P, Cadranel S, Casswall T, et al. Joint ESPGHAN/NASPGHAN Guidelines for the Management of Helicobacter pylori in Children and Adolescents (Update 2016). JPGN. 2017; 64(6): 991–1003. https://doi.org/10.1097/MPG.0000000000001594 |
[6]
. Therefore this study aimed to determine the epidemiology of and factors associated with
Helicobacter pylori infection and proportion requiring treatment among symptomatic children in northwestern Tanzania.
2. Methods
2.1. Study Design, Duration and Study Area
This was cross-section study conducted from December 2021 to April 2022. The study was conducted in the department of Pediatrics and Child Health outpatient clinic in the Bugando Medical Center (BMC), Mwanza -Tanzania.
2.2. Sample Size Estimation and Sampling Technique
A total of 422 children aged 1 to 15 years with gastrointestinal symptoms were enrolled by convenience sampling method. The sample size was estimated by Kish Leslie formula
| [7] | Leslie Kish New York: John Wiley and Sons Inc. Survey Sampling. Am Polit Sci Rev. 1965; 59(4): 643. |
[7]
, using previous prevalence of 42.9% by Jaka
et al | [5] | Jaka H et al. Prevalence and risk factors associated with Helicobacter pylori infections in Tanzanian children. Catholic University of Health and Allied Sciences. 2016. |
[5]
.
2.3. Inclusion Criteria
Children aged 1 to 15 years with one of the gastrointestinal symptoms like abdominal pain, vomiting, nausea, bloating, heartburn, refusal to feed, or restlessness were included.
2.4. Exclusion
Children producing watery stool/diarrhea were excluded. It has been suggested before that unformed or watery stool results to low accuracy of HpSA test due to dilution of
H. pylori specific antigens
.
2.5. Data Collection
Socio-demographic and clinical data were collected using a pre-tested questionnaire. The questionnaire included socio-demographic characteristics such as age and gender of participants, place of residence, school attendance, type of home toilet, sources of drinking water at home, number of people and rooms in their house, family history of peptic ulcers, and the educational level of the parent/guardian. The clinical characteristics such as abdominal pain, vomiting, nausea, bloating, heartburn, passage of dark stool, refusal to feed, or restlessness were recorded. Parents/guardian provided the information on behalf of their children for those who were too young or fail to express themselves. Stadiometer was used to measure height. Body weight was measured using weighing scale. Oxygen saturation was measured by using pulseoxymeter and epigastric/right upper quadrant tenderness was assessed clinically by palpation and observing facial expression and response of participants.
2.6. Sample Collection
Participants were given clean, dry, stool containers and they were instructed to provide small amount size of the peanut stool specimen, and not to contaminate the stool specimen with urine or toilet water during the time of collection. Specimen were taken to the laboratory immediately after collection, for processing by an entitled laboratory technician, to detect the presence of H. pylori antigens.
2.7. Laboratory Procedure
The test based on the principle of lateral flow immunochromatography for qualitative determination of H. pylori antigens in stool that uses H. pylori specific monoclonal antibodies coated on the membrane of the test device Lot: 1909052 manufactured by (Zhejiang orient biotech company China). According to the manufacturer recommendation the test device and samples were allowed to reach room temperature (15–300C) prior to testing. The package was opened when ready to perform the test. Using the applicator stick of the provided sample diluents vial, a small portion (5mm in diameter) of stool specimen was transferred into the sample diluents. Then shaken gently in order to unstuck and facilitate sample dispersion and 4 drops of the sample was added in the test device. Thereafter the result was interpreted at ten to fifteen minutes.
2.8. Upper Gastrointestinal Endoscopy
Due to financial restrictions we managed to do OGD to about 1/2 (55) of those who were H. pylori infected to have a picture on the proportion that required treatment.
Based on endoscopy unit at BMC can only perform upper gastrointestinal endoscopy for the children ≥ 2 years old, due to unavailability of endoscope size for those < 2 years old children. In this study 5 (4.8%) under 2 years old H. pylori infected children were excluded for OGD remaining with 100 children ≥ 2 years old. Randomly 55 H. pylori infected children, were serially selected for OGD by picking their registration number written in folded mixed-up pieces of papers. This was a representative sample in determining the proportion that required treatment. Endoscopies were done by experienced gastroenterologists to the children instructed to fast for 8 hours prior the procedure to prevent aspiration. The visualization of gastric and duodenal mucosal was done using endoscope (EPK-i 5010 manufactured by Pentax medical company Japan).
2.9. Data Quality Control
To ensure internal validity of the study the following precautions were taken into considerations:
The data-collecting tool was pre-tested.
The principal investigator ensured completeness and consistency of edited data collected.
Data was kept confidential under lock and key.
Internal quality controls were included in the test. A colored band appeared in the control region (C) was an internal positive procedural control, confirming sufficient specimen volume and correct procedural technique.
2.10. Data Management and Statistical Data Analysis
Data was entered into Microsoft excel sheet then analyzed using STATA version 15. Continuous variables were summarized as median with interquartile range. Categorical variables were summarized using proportion and percent. Odds ratios with respective 95% confidence interval (CI) were reported and p-value < 0.05 was considered to constitute a statistically significant difference. Furthermore those factors with p-value < 0.05 on univariate analysis method were subjected to multivariate regression model to determine the independent factors associated with H. pylori infection.
3. Results
3.1. Study Enrollment
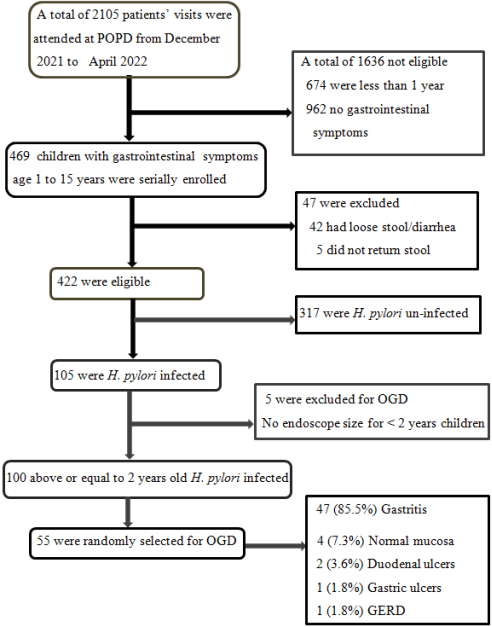
A total of 2105 patients visits were attended at pediatric outpatient department (POPD) clinic, 1636 children were not eligible to be enrolled in the study. Of those who were not eligible 674 (32.0%) were under one year of age, 962 (45.7%) had no gastrointestinal symptoms. About 469 (22.3%) children with gastrointestinal symptoms age 1 to 15 years were serially enrolled in our study, from which 47 participants were excluded of which 42 (1.9%) and 5 (0.2%) did not return stool sample. Remained with 422 participants who were tested for
H. pylori stool antigens, of which 105 (24.9%) were infected. Of the
H. pylori infected 5 (0.05%) children under 2 years of age were excluded for OGD due to unavailability of endoscope size for this age group at Bugando Medical Center. About 55 children were randomly selected from those above or equal to 2 years of age
H. pylori infected for endoscopy. None of the participants were excluded due to lack of consent. Enrollment is described in the recruitment flow chart (
Figure 1).
Figure 1. Recruitment flow chart.
3.2. Demographic and Clinical Characteristics of the Enrolled Participants
The median age was 7 [IQR 3 – 10] years. More than half of the participants (56.4%) were males. Majority of participants (79.4%) resided in urban areas and (70.4%) of all participants were school going. Approximately (90.3%) had flush toilets and (84.6%) used tap water. Minority (4.5%) were from households with more than three members per room. Slightly more than half of the parents (59.2%) had attained beyond primary education level (
Table 1).
More than three quarters (76.1%) of the participant had abdominal pain, followed by vomiting (22.3%), bloating (13.5%), refusal to feed (13.3%), restlessness (10.4%), nausea (8.3%), dark stool (6.9%) and upper quadrant tenderness (2.6%) (
Table 2).
Prevalence of and factors associated with of Helicobacter Pylori infection among symptomatic children aged 1 to 15 years.
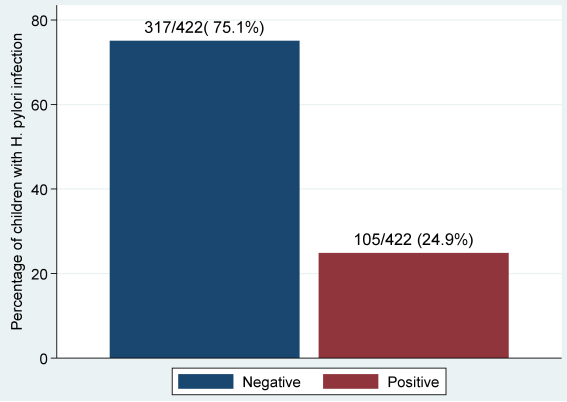
The prevalence of
H. pylori infection was 105 (24.9%) (
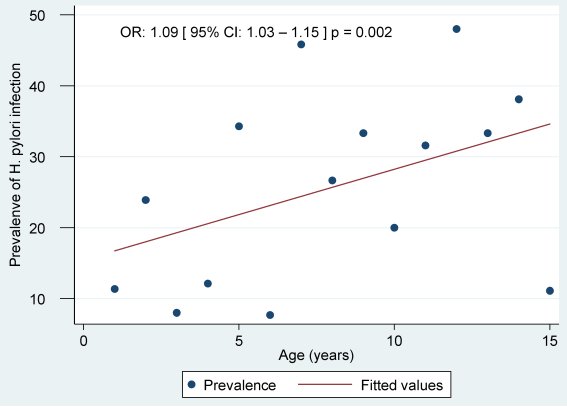
Figure 2). As age increases by 1 year, the risk of
H. pylori infection increases by 9% (OR=1.09; 95%CI 1.03 – 1.15; P=0.002), (
Figure 3). In univariate logistic regression method the factors associated with
H. pylori infection were age (OR=2.5; 95% CI 1.4 – 4.3; P=0.002), and abdominal pain (OR=2.4; 95% CI 1.4 – 4.2], P=0.002). Moreover, abdominal pain (OR=2.2; 95% CI 1.2 – 4.0 P=0.01) and age 11 – 15 years (OR=1.4; 95%CI 1.0 – 1.9; P=0.03) remained independently associated with
H. pylori infection on multivariable analysis, (
Table 3).
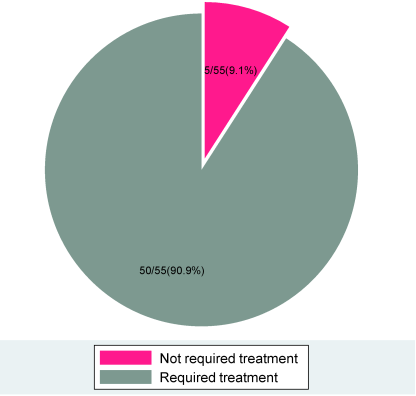
Proportion of Helicobacter pylori infected children that required treatment among symptomatic children aged 1 to 15 years.
Of 100 participants above or equal to 2 years of age,
H. pylori infected children 55 randomly selected children did endoscopy, and 50 (90.9%) among those who had endoscopy done revealed gastrointestinal lesions that warranted treatment (
Figure 4). The median age of the
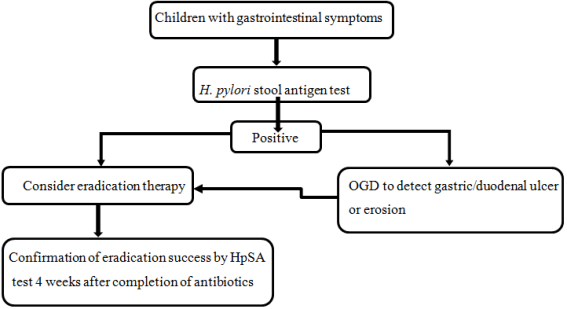
H. pylori infected children who required treatment was 10 [IQR 7 – 13] years. Our study also has suggested an algorithm for the management of children with
H. pylori infection (
Figure 5).
3.3. Pattern of Endoscopic Findings
About 55 (55%) children with
H. pylori infection had endoscopy done. Majority had gastritis 47 (85.5%) that included 28 (50.9%) antral gastritis and 19 (34.5%) pangastritis, followed by 4 (7.3%) with normal mucosa, 2 (3.6%) duodenal ulcers, 1 (1.8%) gastric ulcer and 1 (1.8%) had gastroesophageal reflux disease (
Table 4).
Figure 2. Prevalence of Helicobacter pylori infection among study participants (N = 422).
Figure 3. Prevalence of Helicobacter pylori infection increases with increase in age.
Figure 4. Proportion of Helicobacter pylori infected children who required treatment (N = 55).
Figure 5. Algorithm for the management of children with Helicobacter pylori infection.
Table 1. Demographic and other baseline characteristics of 422 children aged 1 to 15 years attended outpatient clinic at Bugando Medical Centre from December 2021 to April 2022.
Characteristics | Number (%) or Median [IQR]n = 422 |
Gender | |
Male | 238 (56.4) |
Female | 184 (43.6) |
Age in years | 7 [3 – 10] |
Residence | |
Urban | 335 (79.4) |
Rural | 87 (20.6) |
School attendance | |
Yes | 297 (70.4) |
No | 125 (29.6) |
Overcrowding | |
Yes | 19 (4.5) |
No | 403 (95.5) |
Source of water | |
Tap | 357 (84.6) |
Non tap. | 65 (15.4) |
Type of toilet | |
Pit latrine | 41 (9.7) |
Flush toilet | 381 (90.3) |
Education level of the parents | |
≤ 7 years in school | 172 (40.8) |
>7 years in school | 250 (59.2) |
Family history of PUD | |
Yes | 91 (21.6) |
No | 331 (78.4) |
Table 2. Clinical characteristics of study participants (N = 422).
Characteristics | Number (%) or Median [IQR] n = 422 |
Presenting symptoms and signs | |
Abdominal pain | 321 (76.1) |
Vomiting | 94 (22.3) |
Bloating | 57 (13.5) |
Refusal to feed | 56 (13.3) |
Restlessness | 44 (10.4) |
Nausea | 35 (8.3) |
Dark stool | 29 (6.9) |
Upper quadrant tenderness | 11 (2.6) |
Antibiotic use in the past 30 days | 35 (8.3) |
Physical exam findings | |
Saturation Oxygen in percentage | 98 [97 – 99] |
H. pylori positive | 105 (24.9) |
Age H. pylori infected in years | 8 [5 – 12] |
Age H. pylori un-infected in years | 6 [3 – 10] |
Children with gastrointestinal lesions warranted treatment | 50/55 (90.9) |
Age of children required treatment in years | 10 [7 – 13] |
Table 3. Factors associated with Helicobacter pylori infection (N = 422).
Variable | H pylori antigen test | Univariate | Multivariate |
Positive (n=105) | Negative (n=317) | OR [95% CI] | p- value | OR [95%CI] | p-value |
n (%) | n (%) |
Age in years 1 – 5 | 33 (18.1) | 149 (81.9) | 1.0 | | 1.4 [1.0 –1.9] | 0.03 |
6 -10 | 40 (26.9) | 109 (73.1) | 1.7 [0.9 – 2.8] | 0.06 |
11 –15 | 32 (35.2) | 59 (64.8) | 2.5 [1.4 – 4.3] | 0.002 |
Gender Female | 49 (26.6) | 135 (73.4) | 1.0 | |
Male | 56 (23.5) | 182 (76.5) | 1.2 [0.8 – 1.8] | 0.47 |
Residence Rural | 20 (23.0) | 67 (77.0) | 1.0 | |
Urban | 85 (25.4) | 250 (74.6) | 0.9 [0.5 – 1.5] | 0.65 |
School attendance No | 22 (17.6) | 103 (82.4) | 1.0 | |
Yes | 83 (27.9) | 214 (72.1) | 1.8 [1.1 – 3.1] | 0.53 |
Overcrowding No | 103 (25.6) | 300 (74.4) | 1.0 | |
Yes | 2 (10.5) | 17 (89.5) | 0.3 [0.1 – 1.5] | 0.16 |
Source of waterNon tap | 13 (20.0) | 52 (80.0) | 1.0 | |
Tap | 92 (25.8) | 265 (74.2) | 1.4 [0.7 – 2.7] | 0.32 |
Toilet Flush toilet | 97 (25.5) | 284 (74.5) | 1.0 | |
Pit Latrine | 8 (19.5) | 33 (80.5) | 1.4 [0.6 – 3.2] | 0.41 |
Family history PUDNo | 81 (24.4) | 251 (75.6) | 1.0 | |
Yes | 24 (26.7) | 66 (73.3) | 1.1 [0.7 – 1.9] | 0.66 |
Parent education | | | | |
≤ 7 years in school | 38 (22.1) | 134 (77.9) | 1.0 | 0.27 |
> 7 years in school | 67 (26.8) | 183 (73.2) | 1.3 [0.8 – 2.0] |
Abdominal pain No | 11 (10.9) | 90 (89.1) | 1.0 | | 2.2 [1.2– 4.0] | 0.01 |
Yes | 94 (29.3) | 227 (70.7) | 2.4 [1.4 – 4.2] | 0.002 |
Nausea No | 98 (26.4) | 285 (73.6) | 1.0 | |
Yes | 7 (20.0) | 28 (80.0) | 0.8 [0.4 – 1.9] | 0.65 |
Vomiting No | 83 (25.3) | 245 (74.7) | 1.0 | |
Yes | 22 (23.4) | 72 (76.6) | 0.9 [0.5 – 1.6] | 0.70 |
Bloating No | 92 (25.2) | 273 (74.8) | 1.0 | |
Yes | 13 (22.8) | 44 (77.2) | 0.9 [0.5 – 1.7] | 0.69 |
Dark stool No | 95 (24.2) | 298 (75.8) | 1.0 | |
Yes | 10 (34.5) | 19 (65.5) | 1.7 [0.7 – 3.7] | 0.22 |
Refusal to feed No | 94 (25.7) | 272 (74.3) | 1.0 | |
Yes | 11 (19.6) | 45 (80.4) | 0.7 [0.4 – 1.4] | 0.33 |
Restlessness No | 103 (24.6) | 315 (75.4) | 1.0 | |
Yes | 2 (50.0) | 2 (50.0) | 3.1 [0.4 – 21.9] | 0.26 |
Antibiotic use No | 99 (25.6) | 288 (74.4) | 1.0 | |
Yes | 6 (17.1) | 29 (82.9) | 0.6 [0.2 – 1.5] | 0.27 |
Upper- quadrant No | 101 (24.6) | 310 (75.4) | 1.0 | |
tenderness Yes | 4 (36.4) | 7 (63.6) | 1.8 [0.5 – 6.1] | 0.38 |
Table 4. The patterns of endoscopic findings of 55 children aged 1 to 15 years attended outpatient clinic at Bugando Medical Centre from December 2021 to April 2022.
Endoscopic findings | Number (%) n = 55 |
Gastritis | 47 (85.5) |
Normal findings | 4 (7.3) |
Duodenal ulcers | 2 (3.6) |
Gastric ulcer | 1 (1.8) |
Gastroesophageal reflux | 1 (1.8) |
4. Discussion
Our study found that the prevalence of
H. pylori infection was 24.9% among 422 participants aged 1 to 15 years attending at Bugando Medical Center, Mwanza Tanzania. This is similar compared to the study done by Aitila
et al 24.3%
| [1] | Aitila P, Mutyaba M, Okeny S, Ndawula Kasule M, Kasule R, Ssedyabane F, et al. Prevalence and Risk Factors of Helicobacter pylori Infection among Children Aged 1 to 15 Years at Holy Innocents Children’s Hospital, Mbarara, South Western Uganda. J Trop Med. 2019; 93(3): 1–7. eCollection 2019. https://doi.org/10.1155/2019/9303072 |
[1]
, this may be attributed by similar methodology used and age group of participants.
The higher prevalence from our study than that reported by Awuku
et al 14.2% and Kirdy 16.5%
et al | [9] | Awuku YA, Simpong DL, Alhassan IK, Tuoyire DA, Afaa T, Adu P. Prevalence of Helicobacter pylori infection among children living in a rural setting in Sub-Saharan Africa. BMC Public Health. 2017; 17(360): 1–6. https://doi.org/10.1186/s12889-017-4274-z |
| [10] | Kirdy FAL, Rajab M. Helicobacter pylori Infection : Clinical, Endoscopic, and Histological Findings in Lebanese Pediatric Patients. Int J Pediatr. 2020; 2020(4648167): 1–5. eCollection 2020. https://doi.org/10.1155/2020/4648167 |
[9, 10]
may be ascribed by enrollment of smaller sample size of asymptomatic rural children by Awuku
et al, also Kirdy
et al used large sample size, inclusion of infants, different technique used for
H. pylori detection.
Our study found lower prevalence than the study done by Jaka
et al 42.9% and Galal
et al 64.6%
| [5] | Jaka H et al. Prevalence and risk factors associated with Helicobacter pylori infections in Tanzanian children. Catholic University of Health and Allied Sciences. 2016. |
| [11] | Galal YS, Ghobrial CM, Labib JR, Abou-zekri ME. Helicobacter pylori among symptomatic Egyptian children : prevalence, risk factors, and effect on growth. J Egypt Public Health Assoc. 2019; 94(17): 1–8. https://doi.org/10.1186/s42506-019-0017-6 |
[5, 11]
, the difference may be accredited to multicenter study by Jaka
et al | [5] | Jaka H et al. Prevalence and risk factors associated with Helicobacter pylori infections in Tanzanian children. Catholic University of Health and Allied Sciences. 2016. |
[5]
also involvement of large sample size children < 18 years of age in the study by Galal
et al | [11] | Galal YS, Ghobrial CM, Labib JR, Abou-zekri ME. Helicobacter pylori among symptomatic Egyptian children : prevalence, risk factors, and effect on growth. J Egypt Public Health Assoc. 2019; 94(17): 1–8. https://doi.org/10.1186/s42506-019-0017-6 |
[11]
. Also, it may reflect recent improvements in control and transmissions among children. However, the low prevalence in our study would have been attributed to the recruitment of participants with similar geographical characteristics. This could be due to influence by the environment factors on transmission of
H. pylori infection
| [12] | Hastings E V., Yasui Y, Hanington P, Goodman KJ. Community-driven research on environmental sources of H. pylori infection in arctic Canada. Gut Microbes. 2014; 5(5): 606–17. https://doi.org/10.4161/19490976.2014.969639 |
[12]
.
In our study the median age of participants was 7 [IQR 3 – 10] years, risk of
H. pylori infection increases with increase in age (OR= 1.09; 95%CI 1.03 – 1.15; P = 0.002). As age increases by 1 year the risk of
H. pylori infection increases by 9%. This is also supported by Aitila
et al | [1] | Aitila P, Mutyaba M, Okeny S, Ndawula Kasule M, Kasule R, Ssedyabane F, et al. Prevalence and Risk Factors of Helicobacter pylori Infection among Children Aged 1 to 15 Years at Holy Innocents Children’s Hospital, Mbarara, South Western Uganda. J Trop Med. 2019; 93(3): 1–7. eCollection 2019. https://doi.org/10.1155/2019/9303072 |
[1]
they reported the infection rate increase with increase in age. Age > 10 years was independently associated with
H. pylori infection (OR=1.4; 95%CI 1.0 – 1.9; P = 0.03). This is supported by
Galal
et al, Hasosah
et al | [11] | Galal YS, Ghobrial CM, Labib JR, Abou-zekri ME. Helicobacter pylori among symptomatic Egyptian children : prevalence, risk factors, and effect on growth. J Egypt Public Health Assoc. 2019; 94(17): 1–8. https://doi.org/10.1186/s42506-019-0017-6 |
| [13] | Hasosah M, Satti M, Shehzad A, Alsahafi A SG et al. Prevalence and Risk Factors of Helicobacter pylori Infection in Saudi Children: A Three-Year Prospective Controlled Study. Helicobacter. 2015; 20(1): 56–63. https://doi.org/10.1111/hel.12172 |
[11, 13]
. This could be explained by increased children’s contact with the community and outdoor exposure with low knowledge on how to prevent transmissions. Also decreased parental care to these older children.
Abdominal pain occurred frequently 321 (76.1%) among the participant likewise in 95 (90.5%) of those with
H. pylori infection with statistical significance (OR= 2.2; 95%Cl; 1.2 – 4.0; P= 0.01), this was supported by study done by Galal
et al where by 310 (76.2%) among
H. pylori infected had abdominal pain
| [11] | Galal YS, Ghobrial CM, Labib JR, Abou-zekri ME. Helicobacter pylori among symptomatic Egyptian children : prevalence, risk factors, and effect on growth. J Egypt Public Health Assoc. 2019; 94(17): 1–8. https://doi.org/10.1186/s42506-019-0017-6 |
[11]
. Hasosah
et al reported that children with abdominal pain were 2.39 more likely to have
H. pylori infection
| [13] | Hasosah M, Satti M, Shehzad A, Alsahafi A SG et al. Prevalence and Risk Factors of Helicobacter pylori Infection in Saudi Children: A Three-Year Prospective Controlled Study. Helicobacter. 2015; 20(1): 56–63. https://doi.org/10.1111/hel.12172 |
[13]
. This could be explained by inclusion of symptomatic children that could be having gastrointestinal lesion following
H. pylori infection causing these manifestations. Our finding was in contrast to the study by Spee L
et al that reported no association between recurrent abdominal pain and
H. pylori infection in children
| [14] | Spee LAA, Madderom MB, Pijpers M, Van Leeuwen Y, Berger MY. Association between Helicobacter pylori and gastrointestinal symptoms in children. Pediatrics. 2010; 125(3): 651–69. https://doi.org/10.1542/peds.2010-0941 |
[14]
.
This study found that majority of the participants had antral gastritis 28/55 (50.9%) and pangastritis 19 (34.5%) this was supported by a study done by Kirdy
et al which reported that superficial gastritis 46 (43.3%) and nodular gastritis 44 (41.5%) occurred in
H. pylori-positive patients
| [10] | Kirdy FAL, Rajab M. Helicobacter pylori Infection : Clinical, Endoscopic, and Histological Findings in Lebanese Pediatric Patients. Int J Pediatr. 2020; 2020(4648167): 1–5. eCollection 2020. https://doi.org/10.1155/2020/4648167 |
[10]
. Also, Escobar
et al reported that pangastritis in 18 (43.9%) and antral nodular gastritis in 15 (36.6%) among symptomatic
H. pylori-positive Cuban patients
| [15] | Llanes R, Escobar MP, Gala A, Capo V, Pe GI. Low Prevalence of Helicobacter pylori Among Symptomatic Children from a Hospital in Havana, Cuba. J Trop Pediatr Vol. 2012; 58(3): 231–4. https://doi.org/10.1093/tropej/fmr060 |
[15]
. This could be accredited to inclusion of symptomatic children. Our study found 4 (7.3%) had normal endoscopic findings. This could be explained by T cell downregulation of inflammation in children as it has been suggested in a previous study
.
The joint ESPGHAN/NASPGHAN guidelines recommend treatment for
H. pylori infection in children with gastric or duodenal ulceration or erosions
| [6] | Jones NL, Koletzko S, Goodman K, Bontems P, Cadranel S, Casswall T, et al. Joint ESPGHAN/NASPGHAN Guidelines for the Management of Helicobacter pylori in Children and Adolescents (Update 2016). JPGN. 2017; 64(6): 991–1003. https://doi.org/10.1097/MPG.0000000000001594 |
[6]
. American College of Gastroenterology recommend treatment of
H. pylori infection in those with active PUD, confirmed history of PUD (not previously treated for
H. pylori), gastric mucosa associated lymphoid tissue lymphoma (low grade) or after endoscopic resection of early gastric cancer
| [17] | Guidelines ACG. H. pylori Stool Antigen Testing Following the 2017 ACG Guidelines for H. pylori diagnosis. 2018; (1): 1–4. |
[17]
. Of the 55 participants who had endoscopy done 50 (90.9%) revealed lesions that warranted treatment. The median age of the
H. pylori infected children that required treatment was 10 [IQR 7 – 13] years.
5. Limitations of the Study
In our study we did not include infants as it has been suggested before that breastfeeding in infancy lowers the acquisition of H. pylori infection in early life.
About five under two years of age children could not undergo oesophagogastroduodenoscopy due to unavailability of appropriate size endoscope.
Only half of H. pylori infected children did oesophagogastroduodenoscopy, due to my financial restrictions.
In this study we did endoscopic diagnosis of gastritis instead of biopsy as a gold standard.
6. Conclusion
About a quarter of the enrolled children had H. pylori infection. Increase in age and abdominal pain were independently associated with H. pylori infection. Most H. pylori stool antigen test positive children had endoscopic lesions that warranted treatment.
7. Recommendations
Every symptomatic child with H. pylori stool antigen test positive should be treated according to the existing guidelines.
A call upon policy makers to facilitate availability of endoscopy to lower health facilities such as in regional referral hospitals, to exclude complications of H. pylori infection.
Follow up study should be done to determine treatment outcome post-eradication therapy.
Abbreviations
AMR: Antimicrobial Resistance
BMC: Bugando Medical Center
CI: Confidence Interval
CUHAS: Catholic University of Health and Allied Sciences
ESPGHAN: European Society of Pediatric Gastroenterology Hepatology and Nutrition
GERD: Gastroesophageal Reflux Disease
HpSA: Helicobacter pylori Stool Antigen
LMICs: Low and Middle-Income Countries
NASPGHAN: North American Society of Pediatric Gastroenterology Hepatology and Nutrition
OGD: Oesophagogastroduodenoscopy
OR: Odds Ratio
POPD: Pediatric Outpatient Department
PPI: Proton Pump Inhibitors
PUD: Peptic Ulcer Disease
UBT: Urea Breathe Test
Acknowledgments
The authors would like to acknowledge the Ministry of Health for covering the cost of this research. Our heartfelt gratitude goes to the supervisors, the participants and their parents/guardians for their willingnesss to take part in this study and the department of pediatrics and child health, department of internal medicine, endoscopy unit, department of clinical microbiology and immunology of CUHAS, department of clinical biochemistry of CUHAS, clinical laboratory department of BMC and others who contributed for this study. Special thanks to the Catholic University of Health and Allied Sciences-Bugando for the study approval.
Authors Contributions
M. M: Conceived, designed, coordinated the study, wrote the manuscript, performed collection of data, laboratory sample collection, data analysis and interpretation. While H. J., N. K., S. M, D. M, T. M, I. N: Reviewed critically and provided major inputs of the proposal, dissertation and manuscript development; D. M, I. N: Performed endoscopy; B. K, S. M, R. R: Involved in data analysis; E. K: Performed laboratory sample processing.
Funding
Ministry of Health of Tanzania.
Ethical Considerations
Ethical clearance for the study with registration number CREC/512/2021 was obtained from the joint CUHAS/BMC research ethics and review committee. Then the permission for conducting study was obtained from BMC relevant authority. Prior participant’s recruitment, the purpose of the study was explained to the participants and their parents/guardians. Information sheets were provided in Swahili version to ensure understanding by the participants. Participants and their parents/guardians were explained that anesthetic drug would be administered to provide sedation and anesthesia during endoscopic procedure. Also, participants were advised to fast for 8 hours prior the procedure to avoid aspiration during procedure. Participants’ parents/guardians were required to sign a written informed consents form and children > 7 years gave a verbal assent prior their enrollment. Confidentiality was ensured and important findings were shared with clinicians who attend those with H. pylori infection and the endoscopic findings so as to provide appropriate management according to the existing guidelines.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Aitila P, Mutyaba M, Okeny S, Ndawula Kasule M, Kasule R, Ssedyabane F, et al. Prevalence and Risk Factors of Helicobacter pylori Infection among Children Aged 1 to 15 Years at Holy Innocents Children’s Hospital, Mbarara, South Western Uganda. J Trop Med. 2019; 93(3): 1–7. eCollection 2019.
https://doi.org/10.1155/2019/9303072
|
| [2] |
Hooi JKY, Lai WY, Ng WK, Suen MMY, Underwood FE, Tanyingoh D, et al. Global Prevalence of Helicobacter pylori Infection: Systematic Review and Meta-Analysis. Gastroenterology. 2017; 153(2): 420-429.
https://doi.org/10.1053/j.gastro.2017.04.022
|
| [3] |
Salih BA. Helicobacter pylori Infection in Developing Countries : The Burden for How Long ? Saudi J Gastroenterol. 2009; 15(3): 201–207.
https://doi.org/10.4103/1319-3767.54743
|
| [4] |
Bardhan PK. Epidemiological features of Helicobacter pylori infection in developing countries. Clin Infect Dis. 1997; 25(5): 973–8.
https://doi.org/10.1086/516067
|
| [5] |
Jaka H et al. Prevalence and risk factors associated with Helicobacter pylori infections in Tanzanian children. Catholic University of Health and Allied Sciences. 2016.
|
| [6] |
Jones NL, Koletzko S, Goodman K, Bontems P, Cadranel S, Casswall T, et al. Joint ESPGHAN/NASPGHAN Guidelines for the Management of Helicobacter pylori in Children and Adolescents (Update 2016). JPGN. 2017; 64(6): 991–1003.
https://doi.org/10.1097/MPG.0000000000001594
|
| [7] |
Leslie Kish New York: John Wiley and Sons Inc. Survey Sampling. Am Polit Sci Rev. 1965; 59(4): 643.
|
| [8] |
Shimoyama T. Stool antigen tests for the management of Helicobacter pylori infection. World J Gastroenterol. 2013; 19(45): 8188–91.
https://doi.org/10.3748/wjg.v19.i45.8188
|
| [9] |
Awuku YA, Simpong DL, Alhassan IK, Tuoyire DA, Afaa T, Adu P. Prevalence of Helicobacter pylori infection among children living in a rural setting in Sub-Saharan Africa. BMC Public Health. 2017; 17(360): 1–6.
https://doi.org/10.1186/s12889-017-4274-z
|
| [10] |
Kirdy FAL, Rajab M. Helicobacter pylori Infection : Clinical, Endoscopic, and Histological Findings in Lebanese Pediatric Patients. Int J Pediatr. 2020; 2020(4648167): 1–5. eCollection 2020.
https://doi.org/10.1155/2020/4648167
|
| [11] |
Galal YS, Ghobrial CM, Labib JR, Abou-zekri ME. Helicobacter pylori among symptomatic Egyptian children : prevalence, risk factors, and effect on growth. J Egypt Public Health Assoc. 2019; 94(17): 1–8.
https://doi.org/10.1186/s42506-019-0017-6
|
| [12] |
Hastings E V., Yasui Y, Hanington P, Goodman KJ. Community-driven research on environmental sources of H. pylori infection in arctic Canada. Gut Microbes. 2014; 5(5): 606–17.
https://doi.org/10.4161/19490976.2014.969639
|
| [13] |
Hasosah M, Satti M, Shehzad A, Alsahafi A SG et al. Prevalence and Risk Factors of Helicobacter pylori Infection in Saudi Children: A Three-Year Prospective Controlled Study. Helicobacter. 2015; 20(1): 56–63.
https://doi.org/10.1111/hel.12172
|
| [14] |
Spee LAA, Madderom MB, Pijpers M, Van Leeuwen Y, Berger MY. Association between Helicobacter pylori and gastrointestinal symptoms in children. Pediatrics. 2010; 125(3): 651–69.
https://doi.org/10.1542/peds.2010-0941
|
| [15] |
Llanes R, Escobar MP, Gala A, Capo V, Pe GI. Low Prevalence of Helicobacter pylori Among Symptomatic Children from a Hospital in Havana, Cuba. J Trop Pediatr Vol. 2012; 58(3): 231–4.
https://doi.org/10.1093/tropej/fmr060
|
| [16] |
Bagheri N, Salimzadeh L SH. Microbial Pathogenesis. The role of T helper 1-cell response in Helicobacter pylori -infection. Microb Pthogenes. 2018; 123: 1–8.
https://doi.org/10.1016/j.micpath.2018.06.033
|
| [17] |
Guidelines ACG. H. pylori Stool Antigen Testing Following the 2017 ACG Guidelines for H. pylori diagnosis. 2018; (1): 1–4.
|
Cite This Article
-
APA Style
Mkwizu, M., Jaka, H., Mshana, S., Majinge, D., Nkandala, I., et al. (2024). Epidemiology of and Factors Associated with Helicobacter Pylori Infection and Proportion Requiring Treatment Among Symptomatic Children in Northwestern Tanzania. American Journal of Pediatrics, 10(2), 52-62. https://doi.org/10.11648/j.ajp.20241002.12
 Copy
|
Copy
|
 Download
Download
ACS Style
Mkwizu, M.; Jaka, H.; Mshana, S.; Majinge, D.; Nkandala, I., et al. Epidemiology of and Factors Associated with Helicobacter Pylori Infection and Proportion Requiring Treatment Among Symptomatic Children in Northwestern Tanzania. Am. J. Pediatr. 2024, 10(2), 52-62. doi: 10.11648/j.ajp.20241002.12
Copy
|
Download
AMA Style
Mkwizu M, Jaka H, Mshana S, Majinge D, Nkandala I, et al. Epidemiology of and Factors Associated with Helicobacter Pylori Infection and Proportion Requiring Treatment Among Symptomatic Children in Northwestern Tanzania. Am J Pediatr. 2024;10(2):52-62. doi: 10.11648/j.ajp.20241002.12
Copy
|
Download
-
@article{10.11648/j.ajp.20241002.12,
author = {Mwanaidi Mkwizu and Hyasinta Jaka and Stephen Mshana and David Majinge and Igembe Nkandala and Delfina Msanga and Tulla Masoza and Benson Kidenya and Elig Kimosso and Neema Kayange},
title = {Epidemiology of and Factors Associated with Helicobacter Pylori Infection and Proportion Requiring Treatment Among Symptomatic Children in Northwestern Tanzania
},
journal = {American Journal of Pediatrics},
volume = {10},
number = {2},
pages = {52-62},
doi = {10.11648/j.ajp.20241002.12},
url = {https://doi.org/10.11648/j.ajp.20241002.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajp.20241002.12},
abstract = {Background: Helicobacter pylori infection has been reported to affect more than half of the global population. The persistence of H. pylori infection results to chronic gastritis and peptic ulcer disease. Despite this burden there is limited published studies regarding proportion of Helicobacter pylori infected children that require treatment in many settings in low and middle-income countries (LMICs). Therefore this study aimed to determine the epidemiology of and factors associated with Helicobacter pylori infection and proportion requiring treatment among symptomatic children in northwestern Tanzania. Methodology: This was a hospital based cross-sectional study conducted at BMC hospital in Northwestern Tanzania from December 2021 and April 2022 among outpatient children aged 1 to 15 years with gastrointestinal symptoms. The main study outcome (event) was presence of H. pylori infection as evidence by positive stool antigen test. Independent factors associated with H. pylori infection were determined by logistic regression model. The significance level was set at p-value of H. pylori stool antigen test to determine the proportion of children requiring treatment. Results: A total of 422 symptomatic children were included in the study. The median age was 7 [IQR 3 – 10] years. The prevalence of H. pylori infection was 105 (24.9%). More than half of the participants (56.4%) were males. The risk of H. pylori infection was significantly associated with increase in age (OR= 1.09; 95%CI; 1.03 – 1.15; P= 0.002), and abdominal pain (OR=2.2; 95%CI 1.2 – 4.0; P= 0.01). About 55 participants were randomly selected for OGD among 100 children above or equal 2 years of age with positive stool antigen for H. pylori. The majority were found to have lesion warranting treatment. These lesions included gastritis 47 (85.5%), duodenal ulcers 2 (3.6%) and gastric ulcers 1 (1.8%). Conclusion: About a quarter of the enrolled children had H. pylori infection. Increase in age and abdominal pain were independently associated with H. pylori infection. Most H. pylori stool antigen test positive children had endoscopic lesions that warranted treatment. Therefore every H. pylori stool antigen test positive child needs eradication therapy.
},
year = {2024}
}
Copy
|
Download
-
TY - JOUR
T1 - Epidemiology of and Factors Associated with Helicobacter Pylori Infection and Proportion Requiring Treatment Among Symptomatic Children in Northwestern Tanzania
AU - Mwanaidi Mkwizu
AU - Hyasinta Jaka
AU - Stephen Mshana
AU - David Majinge
AU - Igembe Nkandala
AU - Delfina Msanga
AU - Tulla Masoza
AU - Benson Kidenya
AU - Elig Kimosso
AU - Neema Kayange
Y1 - 2024/04/11
PY - 2024
N1 - https://doi.org/10.11648/j.ajp.20241002.12
DO - 10.11648/j.ajp.20241002.12
T2 - American Journal of Pediatrics
JF - American Journal of Pediatrics
JO - American Journal of Pediatrics
SP - 52
EP - 62
PB - Science Publishing Group
SN - 2472-0909
UR - https://doi.org/10.11648/j.ajp.20241002.12
AB - Background: Helicobacter pylori infection has been reported to affect more than half of the global population. The persistence of H. pylori infection results to chronic gastritis and peptic ulcer disease. Despite this burden there is limited published studies regarding proportion of Helicobacter pylori infected children that require treatment in many settings in low and middle-income countries (LMICs). Therefore this study aimed to determine the epidemiology of and factors associated with Helicobacter pylori infection and proportion requiring treatment among symptomatic children in northwestern Tanzania. Methodology: This was a hospital based cross-sectional study conducted at BMC hospital in Northwestern Tanzania from December 2021 and April 2022 among outpatient children aged 1 to 15 years with gastrointestinal symptoms. The main study outcome (event) was presence of H. pylori infection as evidence by positive stool antigen test. Independent factors associated with H. pylori infection were determined by logistic regression model. The significance level was set at p-value of H. pylori stool antigen test to determine the proportion of children requiring treatment. Results: A total of 422 symptomatic children were included in the study. The median age was 7 [IQR 3 – 10] years. The prevalence of H. pylori infection was 105 (24.9%). More than half of the participants (56.4%) were males. The risk of H. pylori infection was significantly associated with increase in age (OR= 1.09; 95%CI; 1.03 – 1.15; P= 0.002), and abdominal pain (OR=2.2; 95%CI 1.2 – 4.0; P= 0.01). About 55 participants were randomly selected for OGD among 100 children above or equal 2 years of age with positive stool antigen for H. pylori. The majority were found to have lesion warranting treatment. These lesions included gastritis 47 (85.5%), duodenal ulcers 2 (3.6%) and gastric ulcers 1 (1.8%). Conclusion: About a quarter of the enrolled children had H. pylori infection. Increase in age and abdominal pain were independently associated with H. pylori infection. Most H. pylori stool antigen test positive children had endoscopic lesions that warranted treatment. Therefore every H. pylori stool antigen test positive child needs eradication therapy.
VL - 10
IS - 2
ER -
Copy
|
Download