Variation of Retinal Vascularisation Post Bevacizumab for Treatment of Type 1 Retinopathy of Prematurity: A Dose Comparison Based on Retinal Fluorescein Angiography
Retinopathy of prematurity (ROP) is increasingly treated with intravitreal bevacizumab (IVB) but consensus on the optimal dose remains to be determined. Peripheral avascular retina (PAR) and fluorescein leakage are recognised sequelae following anti-vascular endothelial growth factor (VEGF) therapy. The impact of IVB dose on the frequency of these outcomes requires further investigation. This study aimed to compare the prevalence of these two findings on fundus fluorescein angiography (FFA) in infants post treatment of ROP with either 0.625 mg or 0.3125 mg IVB. This was a retrospective study of 74 eyes to compare the prevalence of PAR, fluorescein leak and length of temporal retinal vascularisation (LTRV) after receiving IVB as primary therapy for severe ROP. PAR was observed in almost all eyes treated with IVB (P=1). The number of eyes demonstrating fluorescein leak was double in those receiving 0.3125 mg (6 out of 34) compared to 0.625 mg (3 out of 40) though this difference was not statistically significant (OR 2.61, 95% CI 0.50-17.53, P=0.286). Eyes treated with 0.625 mg IVB had a non-significantly greater mean LTRV by 0.37 disc diameters (P=0.573). Despite lacking statistical significance, the doubled fluorescein leakage rate and trend towards lower LTRV in patients receiving 0.3125 mg may warrant caution in high-risk cases.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Retinopathy of Prematurity, Bevacizumab, Dose Comparison Peripheral Avascular Retina
1. Introduction
Retinopathy of prematurity (ROP) is a sight threatening neovascular disorder affecting preterm infants with low gestational age or birth weight.
[1]
Mintz-Hittner HA, Kennedy KA, Chuang AZ, Group B-RC. Efficacy of intravitreal bevacizumab for stage 3+ retinopathy of prematurity. N Engl J Med 2011; 364(7): 603-15.
Despite advances in neonatal and ophthalmic care, it remains a leading cause of preventable childhood blindness.
[1]
Mintz-Hittner HA, Kennedy KA, Chuang AZ, Group B-RC. Efficacy of intravitreal bevacizumab for stage 3+ retinopathy of prematurity. N Engl J Med 2011; 364(7): 603-15.
The efficacy of anti-vascular endothelial growth factor (VEGF) treatment has been established by the BEATROP and RAINBOW studies.
[1]
Mintz-Hittner HA, Kennedy KA, Chuang AZ, Group B-RC. Efficacy of intravitreal bevacizumab for stage 3+ retinopathy of prematurity. N Engl J Med 2011; 364(7): 603-15.
Stahl A, Lepore D, Fielder A, et al. Ranibizumab versus laser therapy for the treatment of very low birthweight infants with retinopathy of prematurity (RAINBOW): an open-label randomised controlled trial. Lancet 2019; 394(10208): 1551-9.
. Compared with laser photocoagulation, anti-VEGF monotherapy produces both improved anatomical and refractive outcomes in posterior ROP disease.
[1]
Mintz-Hittner HA, Kennedy KA, Chuang AZ, Group B-RC. Efficacy of intravitreal bevacizumab for stage 3+ retinopathy of prematurity. N Engl J Med 2011; 364(7): 603-15.
Since the landmark BEATROP study used 0.625 mg bevacizumab, comparable efficacy has been reportedly achieved with lower doses in terms of acute retreatment rates and disease regression.
[3]
Harder BC, von Baltz S, Jonas JB, Schlichtenbrede FC. Intravitreal low-dosage bevacizumab for retinopathy of prematurity. Acta Ophthalmol 2014; 92(6): 577-81.
Khodabande A, Niyousha MR, Roohipoor R. A lower dose of intravitreal bevacizumab effectively treats retinopathy of prematurity. J AAPOS 2016; 20(6): 490-2.
Wallace DK, Kraker RT, Freedman SF, et al. Assessment of Lower Doses of Intravitreous Bevacizumab for Retinopathy of Prematurity: A Phase 1 Dosing Study. JAMA Ophthalmol 2017; 135(6): 654-6.
Hillier RJ, Connor AJ, Shafiq AE. Ultra-low-dose intravitreal bevacizumab for the treatment of retinopathy of prematurity: a case series. Br J Ophthalmol 2018; 102(2): 260-4.
Dikci S, Ceylan OM, Demirel S, Yilmaz T. Which dose of bevacizumab is more effective for the treatment of aggressive posterior retinopathy of prematurity: lower or higher dose? Arq Bras Oftalmol 2018; 81(1): 12-7.
Han J, Kim SE, Lee SC, Lee CS. Low dose versus conventional dose of intravitreal bevacizumab injection for retinopathy of prematurity: a case series with paired-eye comparison. Acta Ophthalmol 2018; 96(4): e475-e8.
However, there is no consensus among ophthalmologists regarding the ideal dose of intravitreal bevacizumab (IVB) for retinopathy of prematurity (ROP) treatment. The competing clinical priorities include minimising potential systemic side-effects while maximising visual outcomes.
[3]
Harder BC, von Baltz S, Jonas JB, Schlichtenbrede FC. Intravitreal low-dosage bevacizumab for retinopathy of prematurity. Acta Ophthalmol 2014; 92(6): 577-81.
Khodabande A, Niyousha MR, Roohipoor R. A lower dose of intravitreal bevacizumab effectively treats retinopathy of prematurity. J AAPOS 2016; 20(6): 490-2.
Wallace DK, Kraker RT, Freedman SF, et al. Assessment of Lower Doses of Intravitreous Bevacizumab for Retinopathy of Prematurity: A Phase 1 Dosing Study. JAMA Ophthalmol 2017; 135(6): 654-6.
Hillier RJ, Connor AJ, Shafiq AE. Ultra-low-dose intravitreal bevacizumab for the treatment of retinopathy of prematurity: a case series. Br J Ophthalmol 2018; 102(2): 260-4.
Dikci S, Ceylan OM, Demirel S, Yilmaz T. Which dose of bevacizumab is more effective for the treatment of aggressive posterior retinopathy of prematurity: lower or higher dose? Arq Bras Oftalmol 2018; 81(1): 12-7.
Han J, Kim SE, Lee SC, Lee CS. Low dose versus conventional dose of intravitreal bevacizumab injection for retinopathy of prematurity: a case series with paired-eye comparison. Acta Ophthalmol 2018; 96(4): e475-e8.
It is well known that peripheral avascular retina (PAR) occurs frequently in eyes treated with anti-VEGF therapy,
[10]
Mintz-Hittner HA, Geloneck MM, Chuang AZ. Clinical Management of Recurrent Retinopathy of Prematurity after Intravitreal Bevacizumab Monotherapy. Ophthalmology 2016; 123(9): 1845-55.
but there is a paucity of research into whether IVB dose influences the frequency and extent of PAR or vascular leakage that may require further treatment. Our study attempted to answer these questions by utilising fundus fluorescein angiography (FFA) to assess the peripheral retinal vasculature following treatment with 0.625 mg versus a reduced dose of 0.3125 mg IVB for ROP.
2. Methods
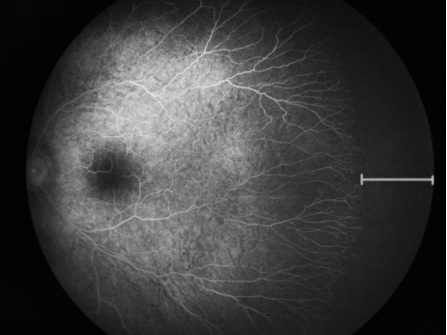
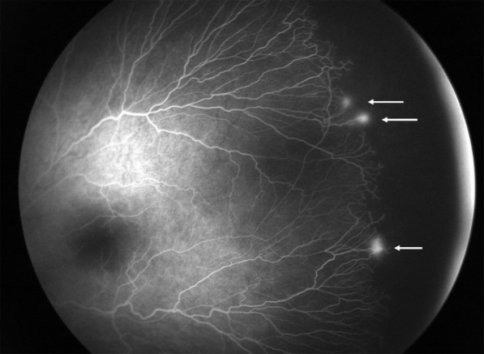
This retrospective cohort study included all infants who underwent FFA imaging post primary IVB therapy for severe ROP (Type 1 ROP and aggressive ROP) between October 2018 and January 2023 at a tertiary paediatric referral centre. Ethics approval was obtained from our institutional Human Research Ethics Committee (EX/2023/QCHQ/94315). Patients were split into Group 1 or 2 and received 0.625 mg or 0.3125 mg IVB respectively. Pre-treatment RetCam images were de-identified and re-graded to confirm treatment requiring ROP by two paediatric ophthalmologists experienced in ROP management. A third paediatric ophthalmologist blinded to treatment groups reviewed the follow-up angiograms for fluorescein leakage and the presence of PAR (Figures 1 and 2). Fluorescein leakage was defined as intense early vascular hyperfluorescence with increased late fluorescence.
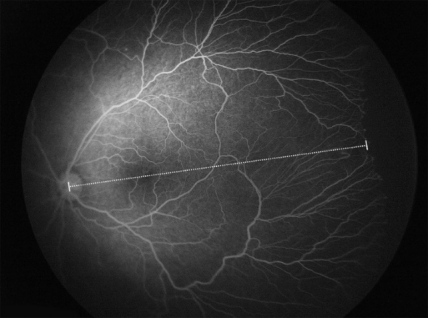
The length of temporal retinal vascularisation (LTRV) was used as a surrogate to gauge retinal vascularisation with a high LTRV indicating less PAR. The LTRV was measured from the optic disc centre through the fovea to the vascular-avascular border using xScope (xScope, version 4.6, The Iconfactory; 2022) as shown in Figure 3. Optic disc diameter (DD) and LTRV were recorded in pixels. To account for differences between sizes of eyes LTRV was compared in DD instead of pixels.
Statistical analyses were performed in RStudio (RStudio, version 2023.03.0+386, R Foundation for Statistical Computing, Vienna, Austria; 2022). Categorical variables were assessed using Fisher’s exact or chi-squared test based on cell counts. The Shapiro-Wilk test for normality was conducted on numerical variables. A Mann-Whitney U test was performed for those with normal distribution and a student’s T-test for the remainder. To compare the difference in LTRV a linear mixed model analysis accounting for inter-eye correlation in bilateral cases was used.
Figure 1. Peripheral avascular retina post 0.3125 mg bevacizumab treatment for retinopathy of prematurity. (GA 25 weeks, BW 800 g and PMA 92 weeks at time of FFA).
Figure 2. Fluorescein leak post 0.3125 mg bevacizumab treatment for retinopathy of prematurity. (GA 23 weeks, BW 526 g and PMA 84 weeks at time of FFA).
Figure 3. Measurement of temporal vascularisation from optic disc through fovea to avascular-vascular border.
3. Results
Eighty-six eyes of 44 infants received IVB during the study period. Seventy-four had FFAs available for review with 40 (54%) having received 0.625 mg bevacizumab. Four from each treatment group were lost to follow-up and four Group 2 eyes did not receive FFA imaging post IVB as they were deemed low risk on indirect ophthalmoscopy. The mean gestational ages (GA) at birth for Group 1 and 2 respectively were 24.3 (range, 23-28) and 24.7 weeks (range, 23-27). Mean birth weights (BW) for Group 1 and 2 were 687.8 (range, 429-1300) and 743.4 g (range, 420-1331).
In Group 1, the mean postmenstrual age (PMA) at time of IVB was 34.9 (range, 32-40) while Group 2 doses were delivered at 35.4 weeks (range, 33-39). Two infants in Group 2 required retreatment one week post initial IVB due to insufficient disease regression. FFAs were performed significantly later in Group 2 at a mean PMA of 94 weeks (range, 42-176) while Group 1 underwent imaging at 74.3 weeks (range, 46-125). Table 1 outlines the baseline characteristics for the two cohorts.
Table 1. Characteristics of Patients Treated with Intravitreal Bevacizumab for Retinopathy of Prematurity.
Characteristic
0.625 mg (40 eyes)
0.3125 mg (34 eyes)
P Value
Mean GA
24.3
24.7
P=0.2921
Mean BW
687.8
743.4
P=0.5937
Sex
M
28 (73.3%)
22 (76.5%)
P=1
F
12
12
AROP
10 (25.0%)
8 (23.5%)
P=0.6122
Zone 1 plus
6 (15.0%)
10 (29.4%)
Zone 2 plus
24 (60.0%)
16 (47.1%)
Mean PMA at Treatment
34.9
35.4
P=0.3514
Mean PMA at FFA
74.3
94.0
P=0.049
Retreatment
0
2 (5.8%)
P=0.4595
PAR was observed in almost all treated eyes with a higher number amongst Group 2 patients (P=1). Group 1 demonstrated a lower rate of fluorescein leak, but this was not statistically significant (OR 2.61, 95% CI 0.50-17.53, P=0.286). Two of three eyes in Group 1 demonstrating fluorescein leak had aggressive ROP and the other belonged to a patient with zone 1 plus disease. Among the six Group 2 eyes, two had zone 1 disease with plus and the remainder were zone 2.
In 67 eyes with FFAs of sufficient quality for measurement, a greater mean LTRV of 0.37 DD was measured in patients who received 0.625 mg bevacizumab however this was not significant (P=0.573). Table 2 compares peripheral retinal findings between the two treatment groups.
Table 2. Fluorescein Angiography Findings Following Different Doses of Intravitreal Bevacizumab for Retinopathy of Prematurity.
Finding
0.625 mg (40 eyes)
0.3125 mg (34 eyes)
P value
Eyes with fluorescein leak
3 (7.5%)
6 (17.6%)
P=0.286
Eyes with peripheral avascular retina
38 (95%)
34 (100%)
P=1
Mean amount of temporal retinal vascularisation in disc diameters (n=67)
12.13 DD
11.76 DD
P=0.573
4. Discussion
Study findings
Our retrospective study compares FFA findings following 0.625 mg versus 0.3125 mg bevacizumab for treatment of ROP. No significant statistical difference in fluorescein leak, PAR and LTRV was found between groups. Notably despite this, double the number of infants had fluorescein leakage in Group 2. Given the small sample size, it is possible the study had insufficient power to detect a significant difference between the two groups.
A higher LTRV was noted in Group 1 infants that received 0.625 mg although the difference was not significant. Due to clinician preference, all Group 1 infants proceeded directly to FFA post IVB without clinic review and were imaged significantly earlier by almost 20 weeks on average. It is possible if Group 1 FFAs were performed later, further vascularisation could have occurred and a statistically difference in retinal vascularisation may be detected. In contrast to our findings, a comparable study by Bayramoglu et al. of 84 eyes also utilising FFA imaging found a lower LTRV in their 0.625 mg group.
[11]
Bayramoglu SE, Sayin N. The Effect of Intravitreal Bevacizumab Dose on Retinal Vascular Progression in Retinopathy of Prematurity. Ophthalmologica 2022; 245(2): 161-172.
Although this result was also statistically non-significant, the authors of that paper acknowledged selection bias may have occurred as their 0.3125 mg group had lower plus disease severity and higher GA.
[11]
Bayramoglu SE, Sayin N. The Effect of Intravitreal Bevacizumab Dose on Retinal Vascular Progression in Retinopathy of Prematurity. Ophthalmologica 2022; 245(2): 161-172.
Clinician use of FFA post anti-VEGF for ROP varies and there is currently no standard practice internationally including Australia.
[12]
Dai S, Elder J, Spargo M, Gole G. Royal Australian and New Zealand College of Ophthalmologists Retinopathy of Prematurity (ROP) Screening and Treatment Guideline. October 2021. Accessed 08 August 2023.
FFA post IVB treatment can help identify ROP sequelae not visualised otherwise.
[13]
Kvopka M, Chan W, Lake SR, et al. Fundus fluorescein angiography imaging of retinopathy of prematurity in infants: A review. Surv Ophthalmol 2023; 68(5): 849-60.
[14]
Mansukhani SA, Hutchinson AK, Neustein R, et al. Fluorescein Angiography in Retinopathy of Prematurity: Comparison of Infants Treated with Bevacizumab to Those with Spontaneous Regression. Ophthalmol Retina 2019; 3(5): 436-43.
Celiker H, Sahin O. Angiographic findings in cases with a history of severe retinopathy of prematurity treated with anti- VEGFs: follow-up to age 6 years. Int Ophthalmol 2021; 42(4): 1317–37.
Where the vascular-avascular junction can be unclear on examination or colour fundus photography, areas of PAR are well-demarcated
[13]
Kvopka M, Chan W, Lake SR, et al. Fundus fluorescein angiography imaging of retinopathy of prematurity in infants: A review. Surv Ophthalmol 2023; 68(5): 849-60.
[15]
Celiker H, Sahin O. Angiographic findings in cases with a history of severe retinopathy of prematurity treated with anti- VEGFs: follow-up to age 6 years. Int Ophthalmol 2021; 42(4): 1317–37.
Mansukhani et al. noted fluorescein leak was present without abnormal vessels on indirect ophthalmoscopy in 40% of patients.
[14]
Mansukhani SA, Hutchinson AK, Neustein R, et al. Fluorescein Angiography in Retinopathy of Prematurity: Comparison of Infants Treated with Bevacizumab to Those with Spontaneous Regression. Ophthalmol Retina 2019; 3(5): 436-43.
To improve diagnostic reliability, FFA has good interoperator concordance in evaluation of leakage and ischaemic retina amongst ophthalmologists with varied expertise.
[13]
Kvopka M, Chan W, Lake SR, et al. Fundus fluorescein angiography imaging of retinopathy of prematurity in infants: A review. Surv Ophthalmol 2023; 68(5): 849-60.
[13]
.
Almost all patients in the study demonstrated PAR on FFA irrespective of IVB dose. The management of PAR following anti-VEGF therapy remains without consensus.
[13]
Kvopka M, Chan W, Lake SR, et al. Fundus fluorescein angiography imaging of retinopathy of prematurity in infants: A review. Surv Ophthalmol 2023; 68(5): 849-60.
[16]
Al-Taie R, Simkin SK, Doucet E, Dai S. Persistent Avascular Retina in Infants With a History of Type 2 Retinopathy of Prematurity: To Treat or Not to Treat? J Pediatr Ophthalmol Strabismus 2019; 56(4): 222-8.
Some clinicians opt to laser all PAR observed on indirect ophthalmoscopy post IVB treatment, others may use FFA as an ancillary tool to aid decision making and ablate eyes with residual PAR or fluorescein leakage.
[13]
Kvopka M, Chan W, Lake SR, et al. Fundus fluorescein angiography imaging of retinopathy of prematurity in infants: A review. Surv Ophthalmol 2023; 68(5): 849-60.
[16]
Al-Taie R, Simkin SK, Doucet E, Dai S. Persistent Avascular Retina in Infants With a History of Type 2 Retinopathy of Prematurity: To Treat or Not to Treat? J Pediatr Ophthalmol Strabismus 2019; 56(4): 222-8.
At our centre, all fluorescein leak post anti-VEGF therapy for ROP is treated using laser. It is debatable if all PAR post anti-VEGF therapy should receive prophylactic laser photocoagulation considering the destructive modality and increased risk for myopia.
[15]
Celiker H, Sahin O. Angiographic findings in cases with a history of severe retinopathy of prematurity treated with anti- VEGFs: follow-up to age 6 years. Int Ophthalmol 2021; 42(4): 1317–37.
Yu Y, Wang J, Chen F, et al. Study protocol for prognosis and treatment strategy of peripheral persistent avascular retina after intravitreal anti-VEGF therapy in retinopathy of prematurity. Trials 2020; 21(1): 493.
A prospective study to determine the two-year outcomes of PAR and fluorescein leakage with or without laser retreatment finished recruitment in January 2022.
[17]
Yu Y, Wang J, Chen F, et al. Study protocol for prognosis and treatment strategy of peripheral persistent avascular retina after intravitreal anti-VEGF therapy in retinopathy of prematurity. Trials 2020; 21(1): 493.
Although ranibizumab was chosen as the anti-VEGF agent, the results when available, could help determine ideal management of these findings.
[17]
Yu Y, Wang J, Chen F, et al. Study protocol for prognosis and treatment strategy of peripheral persistent avascular retina after intravitreal anti-VEGF therapy in retinopathy of prematurity. Trials 2020; 21(1): 493.
Alternatively, as earlier recipients of IVB begin to have long-term follow-up, the results of differing practice preferences will also become available. Notwithstanding this, FFA is an important modality for evaluation of the peripheral retina post IVB, and we would recommend routine use in follow-up.
Limitations
Study limitations in addition to clinician preferences and patient number discussed previously include the retrospective design and small sample size. A larger multi-centre collaboration may help to increase power in future studies examining treatment outcomes in ROP. The effect of attrition bias is likely limited as both treatment groups lost patients to follow-up at a similar rate. As dose of IVB was not chosen based on severity of disease but rather clinician preference, there is low risk of confounding by indication as a result.
In conclusion, our study shows eyes treated with 0.625 mg IVB had increased retinal vascularisation and decreased fluorescein leak however this was not statistically significant. Routine FFA post IVB treatment is recommended for clear visualisation of ROP sequelae and can be useful to guide any retreatment decision.
Abbreviations
BW
Birth Weight
DD
Disc Diameter
FFA
Undus Fluorescein Angiography
GA
Gestational Age
IVB
Intravitreal Bevacizumab
LTRV
Length of Temporal Retinal Vascularisation
PAR
Peripheral Avascular Retina
PMA
Postmenstrual Age
ROP
Retinopathy of Prematurity
VEGF
Vascular Endothelial Growth Factor
Declaration of Funding Sources
None.
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
Mintz-Hittner HA, Kennedy KA, Chuang AZ, Group B-RC. Efficacy of intravitreal bevacizumab for stage 3+ retinopathy of prematurity. N Engl J Med 2011; 364(7): 603-15.
Stahl A, Lepore D, Fielder A, et al. Ranibizumab versus laser therapy for the treatment of very low birthweight infants with retinopathy of prematurity (RAINBOW): an open-label randomised controlled trial. Lancet 2019; 394(10208): 1551-9.
Harder BC, von Baltz S, Jonas JB, Schlichtenbrede FC. Intravitreal low-dosage bevacizumab for retinopathy of prematurity. Acta Ophthalmol 2014; 92(6): 577-81.
Khodabande A, Niyousha MR, Roohipoor R. A lower dose of intravitreal bevacizumab effectively treats retinopathy of prematurity. J AAPOS 2016; 20(6): 490-2.
Wallace DK, Kraker RT, Freedman SF, et al. Assessment of Lower Doses of Intravitreous Bevacizumab for Retinopathy of Prematurity: A Phase 1 Dosing Study. JAMA Ophthalmol 2017; 135(6): 654-6.
Hillier RJ, Connor AJ, Shafiq AE. Ultra-low-dose intravitreal bevacizumab for the treatment of retinopathy of prematurity: a case series. Br J Ophthalmol 2018; 102(2): 260-4.
Dikci S, Ceylan OM, Demirel S, Yilmaz T. Which dose of bevacizumab is more effective for the treatment of aggressive posterior retinopathy of prematurity: lower or higher dose? Arq Bras Oftalmol 2018; 81(1): 12-7.
Han J, Kim SE, Lee SC, Lee CS. Low dose versus conventional dose of intravitreal bevacizumab injection for retinopathy of prematurity: a case series with paired-eye comparison. Acta Ophthalmol 2018; 96(4): e475-e8.
Mintz-Hittner HA, Geloneck MM, Chuang AZ. Clinical Management of Recurrent Retinopathy of Prematurity after Intravitreal Bevacizumab Monotherapy. Ophthalmology 2016; 123(9): 1845-55.
Bayramoglu SE, Sayin N. The Effect of Intravitreal Bevacizumab Dose on Retinal Vascular Progression in Retinopathy of Prematurity. Ophthalmologica 2022; 245(2): 161-172.
Dai S, Elder J, Spargo M, Gole G. Royal Australian and New Zealand College of Ophthalmologists Retinopathy of Prematurity (ROP) Screening and Treatment Guideline. October 2021. Accessed 08 August 2023.
Kvopka M, Chan W, Lake SR, et al. Fundus fluorescein angiography imaging of retinopathy of prematurity in infants: A review. Surv Ophthalmol 2023; 68(5): 849-60.
[14]
Mansukhani SA, Hutchinson AK, Neustein R, et al. Fluorescein Angiography in Retinopathy of Prematurity: Comparison of Infants Treated with Bevacizumab to Those with Spontaneous Regression. Ophthalmol Retina 2019; 3(5): 436-43.
Celiker H, Sahin O. Angiographic findings in cases with a history of severe retinopathy of prematurity treated with anti- VEGFs: follow-up to age 6 years. Int Ophthalmol 2021; 42(4): 1317–37.
Al-Taie R, Simkin SK, Doucet E, Dai S. Persistent Avascular Retina in Infants With a History of Type 2 Retinopathy of Prematurity: To Treat or Not to Treat? J Pediatr Ophthalmol Strabismus 2019; 56(4): 222-8.
Yu Y, Wang J, Chen F, et al. Study protocol for prognosis and treatment strategy of peripheral persistent avascular retina after intravitreal anti-VEGF therapy in retinopathy of prematurity. Trials 2020; 21(1): 493.
Liu, C. Y., FRANZCO, N. B., FRANZCO, S. S., FRANZCO, S. D. (2025). Variation of Retinal Vascularisation Post Bevacizumab for Treatment of Type 1 Retinopathy of Prematurity: A Dose Comparison Based on Retinal Fluorescein Angiography. Clinical Medicine Research, 14(3), 85-89. https://doi.org/10.11648/j.cmr.20251403.16
Liu, C. Y.; FRANZCO, N. B.; FRANZCO, S. S.; FRANZCO, S. D. Variation of Retinal Vascularisation Post Bevacizumab for Treatment of Type 1 Retinopathy of Prematurity: A Dose Comparison Based on Retinal Fluorescein Angiography. Clin. Med. Res.2025, 14(3), 85-89. doi: 10.11648/j.cmr.20251403.16
Liu CY, FRANZCO NB, FRANZCO SS, FRANZCO SD. Variation of Retinal Vascularisation Post Bevacizumab for Treatment of Type 1 Retinopathy of Prematurity: A Dose Comparison Based on Retinal Fluorescein Angiography. Clin Med Res. 2025;14(3):85-89. doi: 10.11648/j.cmr.20251403.16
@article{10.11648/j.cmr.20251403.16,
author = {Cindy Yue-Ying Liu and Nader Beshay FRANZCO and Shaheen Shah FRANZCO and Shuan Dai FRANZCO},
title = {Variation of Retinal Vascularisation Post Bevacizumab for Treatment of Type 1 Retinopathy of Prematurity: A Dose Comparison Based on Retinal Fluorescein Angiography
},
journal = {Clinical Medicine Research},
volume = {14},
number = {3},
pages = {85-89},
doi = {10.11648/j.cmr.20251403.16},
url = {https://doi.org/10.11648/j.cmr.20251403.16},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cmr.20251403.16},
abstract = {Retinopathy of prematurity (ROP) is increasingly treated with intravitreal bevacizumab (IVB) but consensus on the optimal dose remains to be determined. Peripheral avascular retina (PAR) and fluorescein leakage are recognised sequelae following anti-vascular endothelial growth factor (VEGF) therapy. The impact of IVB dose on the frequency of these outcomes requires further investigation. This study aimed to compare the prevalence of these two findings on fundus fluorescein angiography (FFA) in infants post treatment of ROP with either 0.625 mg or 0.3125 mg IVB. This was a retrospective study of 74 eyes to compare the prevalence of PAR, fluorescein leak and length of temporal retinal vascularisation (LTRV) after receiving IVB as primary therapy for severe ROP. PAR was observed in almost all eyes treated with IVB (P=1). The number of eyes demonstrating fluorescein leak was double in those receiving 0.3125 mg (6 out of 34) compared to 0.625 mg (3 out of 40) though this difference was not statistically significant (OR 2.61, 95% CI 0.50-17.53, P=0.286). Eyes treated with 0.625 mg IVB had a non-significantly greater mean LTRV by 0.37 disc diameters (P=0.573). Despite lacking statistical significance, the doubled fluorescein leakage rate and trend towards lower LTRV in patients receiving 0.3125 mg may warrant caution in high-risk cases.
},
year = {2025}
}
TY - JOUR
T1 - Variation of Retinal Vascularisation Post Bevacizumab for Treatment of Type 1 Retinopathy of Prematurity: A Dose Comparison Based on Retinal Fluorescein Angiography
AU - Cindy Yue-Ying Liu
AU - Nader Beshay FRANZCO
AU - Shaheen Shah FRANZCO
AU - Shuan Dai FRANZCO
Y1 - 2025/06/19
PY - 2025
N1 - https://doi.org/10.11648/j.cmr.20251403.16
DO - 10.11648/j.cmr.20251403.16
T2 - Clinical Medicine Research
JF - Clinical Medicine Research
JO - Clinical Medicine Research
SP - 85
EP - 89
PB - Science Publishing Group
SN - 2326-9057
UR - https://doi.org/10.11648/j.cmr.20251403.16
AB - Retinopathy of prematurity (ROP) is increasingly treated with intravitreal bevacizumab (IVB) but consensus on the optimal dose remains to be determined. Peripheral avascular retina (PAR) and fluorescein leakage are recognised sequelae following anti-vascular endothelial growth factor (VEGF) therapy. The impact of IVB dose on the frequency of these outcomes requires further investigation. This study aimed to compare the prevalence of these two findings on fundus fluorescein angiography (FFA) in infants post treatment of ROP with either 0.625 mg or 0.3125 mg IVB. This was a retrospective study of 74 eyes to compare the prevalence of PAR, fluorescein leak and length of temporal retinal vascularisation (LTRV) after receiving IVB as primary therapy for severe ROP. PAR was observed in almost all eyes treated with IVB (P=1). The number of eyes demonstrating fluorescein leak was double in those receiving 0.3125 mg (6 out of 34) compared to 0.625 mg (3 out of 40) though this difference was not statistically significant (OR 2.61, 95% CI 0.50-17.53, P=0.286). Eyes treated with 0.625 mg IVB had a non-significantly greater mean LTRV by 0.37 disc diameters (P=0.573). Despite lacking statistical significance, the doubled fluorescein leakage rate and trend towards lower LTRV in patients receiving 0.3125 mg may warrant caution in high-risk cases.
VL - 14
IS - 3
ER -
Department of Ophthalmology, Queensland Children's Hospital, Brisbane, Australia
Shaheen Shah FRANZCO
Department of Ophthalmology, Queensland Children's Hospital, Brisbane, Australia
Shuan Dai FRANZCO
Department of Ophthalmology, Queensland Children's Hospital, Brisbane, Australia; Faculty of Medicine, The University of Queensland, Brisbane, Australia; Menzies Health Institute Queensland, Griffith University, Brisbane, Australia
Liu, C. Y., FRANZCO, N. B., FRANZCO, S. S., FRANZCO, S. D. (2025). Variation of Retinal Vascularisation Post Bevacizumab for Treatment of Type 1 Retinopathy of Prematurity: A Dose Comparison Based on Retinal Fluorescein Angiography. Clinical Medicine Research, 14(3), 85-89. https://doi.org/10.11648/j.cmr.20251403.16
Liu, C. Y.; FRANZCO, N. B.; FRANZCO, S. S.; FRANZCO, S. D. Variation of Retinal Vascularisation Post Bevacizumab for Treatment of Type 1 Retinopathy of Prematurity: A Dose Comparison Based on Retinal Fluorescein Angiography. Clin. Med. Res.2025, 14(3), 85-89. doi: 10.11648/j.cmr.20251403.16
Liu CY, FRANZCO NB, FRANZCO SS, FRANZCO SD. Variation of Retinal Vascularisation Post Bevacizumab for Treatment of Type 1 Retinopathy of Prematurity: A Dose Comparison Based on Retinal Fluorescein Angiography. Clin Med Res. 2025;14(3):85-89. doi: 10.11648/j.cmr.20251403.16
@article{10.11648/j.cmr.20251403.16,
author = {Cindy Yue-Ying Liu and Nader Beshay FRANZCO and Shaheen Shah FRANZCO and Shuan Dai FRANZCO},
title = {Variation of Retinal Vascularisation Post Bevacizumab for Treatment of Type 1 Retinopathy of Prematurity: A Dose Comparison Based on Retinal Fluorescein Angiography
},
journal = {Clinical Medicine Research},
volume = {14},
number = {3},
pages = {85-89},
doi = {10.11648/j.cmr.20251403.16},
url = {https://doi.org/10.11648/j.cmr.20251403.16},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cmr.20251403.16},
abstract = {Retinopathy of prematurity (ROP) is increasingly treated with intravitreal bevacizumab (IVB) but consensus on the optimal dose remains to be determined. Peripheral avascular retina (PAR) and fluorescein leakage are recognised sequelae following anti-vascular endothelial growth factor (VEGF) therapy. The impact of IVB dose on the frequency of these outcomes requires further investigation. This study aimed to compare the prevalence of these two findings on fundus fluorescein angiography (FFA) in infants post treatment of ROP with either 0.625 mg or 0.3125 mg IVB. This was a retrospective study of 74 eyes to compare the prevalence of PAR, fluorescein leak and length of temporal retinal vascularisation (LTRV) after receiving IVB as primary therapy for severe ROP. PAR was observed in almost all eyes treated with IVB (P=1). The number of eyes demonstrating fluorescein leak was double in those receiving 0.3125 mg (6 out of 34) compared to 0.625 mg (3 out of 40) though this difference was not statistically significant (OR 2.61, 95% CI 0.50-17.53, P=0.286). Eyes treated with 0.625 mg IVB had a non-significantly greater mean LTRV by 0.37 disc diameters (P=0.573). Despite lacking statistical significance, the doubled fluorescein leakage rate and trend towards lower LTRV in patients receiving 0.3125 mg may warrant caution in high-risk cases.
},
year = {2025}
}
TY - JOUR
T1 - Variation of Retinal Vascularisation Post Bevacizumab for Treatment of Type 1 Retinopathy of Prematurity: A Dose Comparison Based on Retinal Fluorescein Angiography
AU - Cindy Yue-Ying Liu
AU - Nader Beshay FRANZCO
AU - Shaheen Shah FRANZCO
AU - Shuan Dai FRANZCO
Y1 - 2025/06/19
PY - 2025
N1 - https://doi.org/10.11648/j.cmr.20251403.16
DO - 10.11648/j.cmr.20251403.16
T2 - Clinical Medicine Research
JF - Clinical Medicine Research
JO - Clinical Medicine Research
SP - 85
EP - 89
PB - Science Publishing Group
SN - 2326-9057
UR - https://doi.org/10.11648/j.cmr.20251403.16
AB - Retinopathy of prematurity (ROP) is increasingly treated with intravitreal bevacizumab (IVB) but consensus on the optimal dose remains to be determined. Peripheral avascular retina (PAR) and fluorescein leakage are recognised sequelae following anti-vascular endothelial growth factor (VEGF) therapy. The impact of IVB dose on the frequency of these outcomes requires further investigation. This study aimed to compare the prevalence of these two findings on fundus fluorescein angiography (FFA) in infants post treatment of ROP with either 0.625 mg or 0.3125 mg IVB. This was a retrospective study of 74 eyes to compare the prevalence of PAR, fluorescein leak and length of temporal retinal vascularisation (LTRV) after receiving IVB as primary therapy for severe ROP. PAR was observed in almost all eyes treated with IVB (P=1). The number of eyes demonstrating fluorescein leak was double in those receiving 0.3125 mg (6 out of 34) compared to 0.625 mg (3 out of 40) though this difference was not statistically significant (OR 2.61, 95% CI 0.50-17.53, P=0.286). Eyes treated with 0.625 mg IVB had a non-significantly greater mean LTRV by 0.37 disc diameters (P=0.573). Despite lacking statistical significance, the doubled fluorescein leakage rate and trend towards lower LTRV in patients receiving 0.3125 mg may warrant caution in high-risk cases.
VL - 14
IS - 3
ER -