Abstract
Background: In Ivory Coast, as in many tropical regions, there is a significant coexistence of infectious diseases and non-communicable diseases (NCDs), particularly within the field of neurology. The dual burden of neuroinfectious diseases, including meningitis and strokes, plays a crucial role in shaping public health strategies implemented by the World Health Organization (WHO) and national health programs. Unfortunately, the epidemiological trends are not regularly updated. This study aims to provide insights into hospital admissions and mortality related to strokes and brain infections to inform health policies and improve disease management. Method: It was a retrospective study that examined the medical records of patients admitted to the neurology department of the Cocody University Hospital in Abidjan from January 1, 2020, to December 31, 2023, and included individuals across all age groups who were diagnosed with stroke, brain abscess, meningitis, or encephalitis. Results: The study involved 1,518 patients, strokes were more common among older adults, with an average age of 57.3 ± 13.7 years. Strokes represented the primary reason for hospitalization, making up 69% of cases, with an annual growth rate of approximately 2%, while neuroinfectious diseases accounted for 13% of total admissions. In-hospital mortality rates were 15% for stroke patients and 28% for those with neuroinfectious diseases, the latter showing a significantly higher mortality risk (odds ratio = 2.50; p < 0.001). Conclusion: Strokes are the leading cause of hospital admissions in our department, with increasing rates; however, neuroinfectious diseases have higher and stable mortality rates, indicating a more severe prognosis. Therefore, health policies must be reassessed to improve prevention and management for both diseases.
Keywords
Epidemiological Trends, Stroke, Neuroinfectious Disease, Abidjan, Tropical Region
1. Introduction
Ivory Coast faces a complex array of health challenges, marked by the simultaneous presence of both communicable and non-communicable diseases (NCDs). In the field of neurology, there are alarming mortality rates linked to strokes and infectious diseases that impact the central nervous system, such as meningitis and encephalitis. Current research indicates a declining incidence of infectious and deficiency-related diseases, alongside a rise in chronic non-communicable diseases, particularly cerebrovascular conditions, including strokes. This situation is often referred to as the "epidemiological transition."
.
Strokes are the second leading cause of death worldwide, accounting for approximately 11.6% of all fatalities. According to the World Health Organization (WHO), 85% of these deaths occur in low- and middle-income countries
| [1] | Wahdan MH. The epidemiological transition. EMHJ - Eastern Mediterranean Health Journal, 2 (1), 8-20, 1996. Published online 1996. Accessed August 25, 2024. https://iris.who.int/handle/10665/118829 |
| [2] | GBD 2019 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021; 20(10): 795-820. https://doi.org/10.1016/S1474-4422(21)00252-0 |
[1, 2]
. In Africa, data from the past ten years indicate that the annual incidence of strokes may reach 316 per 100,000 person-years
, with a 30-day mortality rate that fluctuates between 16.2% and 46%
| [4] | Maredza M, Bertram MY, Tollman SM. Disease burden of stroke in rural South Africa: an estimate of incidence, mortality and disability adjusted life years. BMC Neurol. 2015; 15: 54. https://doi.org/10.1186/s12883-015-0311-7 |
| [5] | Lekoubou A, Nkoke C, Dzudie A, Kengne AP. Stroke admission and case-fatality in an urban medical unit in sub-Saharan Africa: a fourteen year trend study from 1999 to 2012. J Neurol Sci. 2015; 350(1-2): 24-32. https://doi.org/10.1016/j.jns.2015.02.002 |
[4, 5]
. Additionally, neuroinfectious diseases, such as bacterial meningitis and encephalitis, significantly contribute to both mortality and disability-adjusted life years (DALYs) in Africa
. The emergence and re-emergence of infectious with neurological manifestation diseases present escalating public health challenges globally, driven by various factors that facilitate their spread, including climate change, increased vulnerability of hosts, and dynamics associated with pathogens
. Neurological infections are associated with immediate neurological disorders during their acute phase; however, they also play a significant role in the development of long-term consequences, including neurodevelopmental disorders, cerebrovascular diseases, epilepsy, and cognitive impairments
.
The theory of epidemiological transition, introduced by Abdel Omran in 1971, provides a framework for understanding changes in population health dynamics. It indicates that as societies progress and modernize, the primary causes of death evolve from infectious diseases to chronic and degenerative illnesses. This transition is influenced by various factors, including industrialization, improvements in sanitation, and shifts in lifestyle behaviors. During the late 1970s, there was a widespread belief in the notion of the "end of infectious diseases," largely due to breakthroughs in medical and public health practices. However, the later emergence of new infectious pathogens, the rise of antibiotic-resistant bacteria, and the recognition of connections between certain infectious agents and chronic diseases have led to the declaration of a "revival of infectious diseases
. This theory has been subjected to considerable critique and disproof, particularly in tropical settings where infectious diseases such as tuberculosis and HIV are prevalent alongside non-infectious ailments like cardiovascular diseases
| [10] | Desenclos JC, De Valk H. [Emergent infectious diseases: importance for public health, epidemiology, promoting factors, and prevention]. Med Mal Infect. 2005; 35(2): 49-61. https://doi.org/10.1016/j.medmal.2004.09.005 |
[10]
. It is now recognized that the health patterns observed in a society are influenced by a wide range of factors, including demographic, socio-economic, technological, cultural, ecological, and biological changes. As a result, the epidemiological trends is no longer regarded as a linear process but rather as a complex and evolving phenomenon that acknowledges the continuous interaction between infectious and non-infectious diseases in shaping the health of populations
| [10] | Desenclos JC, De Valk H. [Emergent infectious diseases: importance for public health, epidemiology, promoting factors, and prevention]. Med Mal Infect. 2005; 35(2): 49-61. https://doi.org/10.1016/j.medmal.2004.09.005 |
[10]
.
In the early 2000s, the neurology department at COCODY University Hospital reported that neuroinfectious diseases were the primary contributors to hospitalization and mortality, representing 46% of admissions and 23% of deaths
. Strokes were the next most significant cause, representing 43.3% of admissions and 21% of fatalities
. Nevertheless, following that period, there has been a lack of additional research aimed at examining the temporal variations concerning the frequency and mortality rates of strokes in relation to infectious diseases that impact the central nervous system.
The aim of this study is to present significant data regarding the temporal variations of strokes and neuroinfectious diseases within the largest neurology department in the country. This information may prove essential in guiding public health strategies and enhancing the quality of care provided to patients affected by these neurological disorders.
2. Materials and Methods
2.1. Study Design
This study was a retrospective analysis covering a four-year timeframe, from January 2020 to December 2023. It was carried out in the neurology department of COCODY University Hospital, the largest neurology department in Ivory Coast, and it included all patients who were admitted for stroke, meningitis, meningoencephalitis, and brain abscess.
2.2. Study Area and Setting
The study was carried out at the Cocody University Hospital, located in Abidjan, the economic capital of Ivory Coast and the most populous city in French-speaking West Africa. The city is undergoing significant growth, marked by rapid industrialization and urban development. Cocody University Hospital is adjacent to Félix Houphouët-Boigny University and is particularly focused on medical teaching and research. It offers 19 clinical specialties, including neurology. The neurology service consists of around 40 beds and accommodates approximately 550 patients each year. This department is organized into three units: an outpatient consultation unit, a general and vascular neurology inpatient unit, and a neurophysiological exploration unit. This study was conducted within the general and vascular neurology inpatient units.
2.3. Sampling Strategy and Sample Size
The majority of patients are referred from the medical emergency service and outpatient neurology consultations, while a smaller number are transferred from other specialized departments. This study encompassed all patients who were admitted to the neurology department throughout the designated study period and had received a diagnosis of stroke, meningitis, encephalitis, or meningoencephalitis, provided they possessed a comprehensive medical record.
The operational definitions for each diagnosis have been established as follows: stroke is defined as a patient who has experienced an abrupt neurological deficit, for whom a cranial computed tomography (CT) scan or magnetic resonance imaging (MRI) has been conducted, confirming the presence of either ischemic or hemorrhagic stroke. Neuroinfectious diseases encompass all infections that impact the meninges and/or the brain, leading to clinical manifestations such as meningitis, meningoencephalitis, or brain abscess. A definitive diagnosis is established through clinical findings (the patient exhibiting symptoms of meningeal irritation, encephalitis, or intracranial hypertension in conjunction with an infectious syndrome), neuroradiological assessments (cranial CT or MRI), and biological analyses [notable abnormalities in cerebrospinal fluid (CSF) during cytobacteriological examination alongside signs of biological inflammation].
The study excluded patients who had incomplete medical records, those without a conclusive diagnosis at discharge, individuals experiencing both stroke and neuroinfectious conditions simultaneously, and patients showing symptoms suggestive of neuroinfectious disease who either did not receive a lumbar puncture or had a cerebrospinal fluid analysis that returned normal cytobacteriological results.
2.4. Data Collection
Data collection was conducted using a structured form, with primary sources including admission registers and patient records. The gathered information included various variables: the age and sex of patients, their place of origin, the complaints presented upon admission, the mechanisms of lesions, the etiological diagnoses, the definitive diagnoses, the methods of discharge, and the length of hospital stay.
2.5. Data Analysis
Data were compiled in Microsoft Excel 2016 and later imported into R-4.4.1 for analysis. The analysis encompassed all instances of cerebrovascular accidents (strokes) and neuroinfectious diseases recorded during the study timeframe, facilitating the calculation of admission rates and mortality associated with each category of disease. Qualitative variables were expressed as proportions, while continuous variables were evaluated through their mean values. Each independent variable was subjected to univariate logistic regression, with those yielding a p-value of 0.05 or less being further examined through multivariate logistic regression. An independent variable with a p-value under 0.05 was identified as a significant predictor of the discharge modality.
2.6. Ethical Consideration
Ethical approval for this research was sought from the research and ethics committee of Félix Houphouët-Boigny University. Additionally, a request for access to the archives was submitted to the General Director of the Cocody University Hospital, as well as to the head of the neurology department. The collection and analysis of data were conducted in accordance with the principles of anonymity and the Declaration of Helsinki.
3. Results
3.1. Study Population
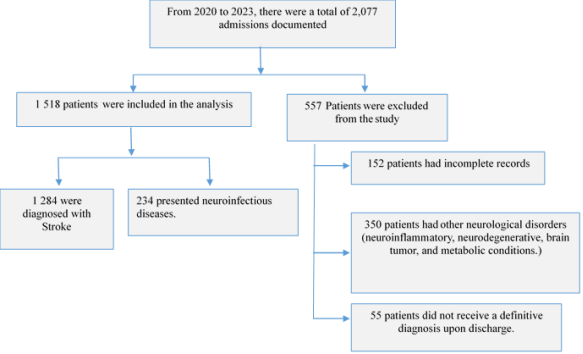
From January 1, 2020, to December 31, 2023, the neurology service at COCODY University Hospital recorded a total of 2,077 patients. Of these, 152 records were incomplete, and 55 patients were discharged without a definitive diagnosis, resulting in their exclusion from the research. Ultimately, 1,868 patients had complete records and a diagnosis at discharge, with 1,284 (69%) diagnosed with stroke, 234 (13%) with neuroinfectious diseases, and 350 (18%) with various other neurological disorders, including neuroinflammatory, neurodegenerative, tumor-related, and metabolic conditions, which were also excluded from the analysis. Therefore, the study concentrated on the 1,518 patients who were admitted specifically for strokes and neuroinfectious diseases.
Figure 1. The patient selection process.
3.2. The Sociodemographic Features of the Patient Within the Two Disease Groups
Table 1. Distribution of socio-demographic characteristics of the study participants.
Patients’ characteristics | Stroke (n, %) | Neuroinfectious diseases (n, %) | Total (n, %) |
Age (year) | | | |
< 20 | 12 (0.9) | 17 (7.2) | 29 (1.9) |
20-40 | 120 (9.3) | 76 (32.4) | 196 (12.9) |
40-60 | 568 (44.2) | 110 (47.0) | 678 (44.6) |
60-80 | 517 (40.2) | 28 (11.9) | 545 (35.9) |
>80 | 67 (5.2) | 3 (1%) | 70 (4.6) |
Mean (standard deviation) | 57.3 ± 13.7 | 44.4 ± 28.8 | |
Gender |
Male | 688 (53.5) | 107 (45.7) | 795 (52.3) |
Female | 596 (46.4) | 127 (54.2) | 723 (47.6) |
Origin |
Rural | 272 (21.1) | 44 (18.8) | 316 (20.8) |
Urban | 1012 (78.8) | 190 (81.1) | 1102 (72.5) |
The average age of patients admitted for a stroke was 57.3 ± 13.7 years, whereas those hospitalized for neuroinfectious diseases had an average age of 44.4 ± 28.8 years. In both disease groups, the gender ratio is approximately 1.1, with a slight predominance of males in stroke cases, accounting for 53.5%, and a slight predominance of females in neuroinfectious disease cases, at 54.2%. Approximately 80% of the patients originate from urban and suburban areas.
3.3. Trend in Stroke Hospital Admissions
In the study period, the majority of patients admitted to our department were those affected by strokes, with a total of 1,284 cases, representing 85% of all admissions. A cumulative increase of 6.6% in stroke cases was observed over four years, corresponding to an average annual increase of approximately 2.2%. Ischemic strokes were the most common, accounting for 56.4% of the total cases, while a significant annual increase in hemorrhagic strokes was noted, reaching about 5.2%. Additionally, there was a general decline in stroke cases among female patients, whereas the incidence of strokes in male patients rose by 13.0% during the study period.
Table 2. Trends in stroke admission from 2020 to 2023 (N= 1,284).
Years | Ischemic Stroke (N, %) | Hemorrhagic Stroke (N, %) | Total stroke per year (N, %) |
Male | Female | Total | Male | Female | Total | Male | Female | Total |
2020 | 87 (50.2) | 88 (49.7) | 175 (24.3) | 53 (47.3) | 59 (52.6) | 112 (20) | 140 (48.7) | 147 (51.2) | 287 (22.3) |
2021 | 83 (51) | 78 (48) | 161 (22.4) | 91 (61.4) | 57 (38.5) | 148 (26.4) | 174 (56.3) | 135 (47.6) | 309 (24.0) |
2022 | 111 (51.6) | 104 (48.3) | 215 (29.2) | 77 (53.4) | 67 (46.2) | 144 (25.8) | 188 (52.3) | 171 (47.6) | 359 (27.9) |
2023 | 92 (52.8) | 82 (46.8) | 174 (24.0) | 93 (60.3) | 61 (39.3) | 155 (27.6) | 186 (56.5) | 143 (43.4) | 329 (25.6) |
Total | 373 (51.4) | 352 (48.5) | 725 (100) | 314 (56.1) | 244 (43.6) | 559 (100) | 688 (53.2) | 596 (46.7) | 1284 (100) |
Trend (%) | -1,1 | -1,3 | -3,76 | 9,1 | 0,55 | 5,2 | 4,0 | -1.3 | 2,2 |
3.4. Trend in Neuroinfectious Diseases Hospital Admissions
Table 3. Trends in neuroinfectious diseases admission from 2020 to 2023 (N= 234).
Year | Brain abscesses (N, %) | Meningoencephalitis (N, %) | Meningitis (N, %) | Total (N, %) |
Male | Female | Total | Male | Female | Total | Male | Female | Total | Male | Female | Total |
2020 | 21 (55.2) | 17 (44.7) | 38 (30.1) | 8 (33.3) | 16 (66.6) | 24 (30.3) | 4 (80) | 1 (20) | 5 (17.2) | 33 (49.2) | 34 (50.7) | 67 (28.6) |
2021 | 11 (35.4) | 20 (64.5) | 31 (24.6) | 7 (58.3) | 5 (41.6) | 12 (15.1) | 4 (44.4) | 5 (55.5) | 9 (31.0) | 22 (42.3) | 30 (57.6) | 52 (22.2) |
2022 | 12 (36.3) | 21 (63.6) | 33 (26.1) | 13 (46.4) | 15 (53.5) | 28 (35.4) | 0 (0) | 5 (100) | 5 (17.2) | 25 (37.8) | 41 (62.1) | 66 (28.2) |
2023 | 15 (62.5) | 09 (37.5) | 24 (19.0) | 5 (33.3) | 10 (66.6) | 15 (18.9) | 7 (70) | 3 (30) | 10 (34.4) | 27 (55.1) | 22 (44.8) | 49 (20.9) |
Total | 59 (46.8) | 67 (53.1) | 126 (100) | 33 (41.7) | 46 (58.2) | 79 (100) | 15 (51.7) | 14 (48) | 29 (100) | 107 (45.7) | 127 (54.2) | 234 (100) |
Trend (%) | -5.3 | -11.5 | -13.8 | -5.3 | -11.5 | -10.6 | 200 | 120 | 45 | -0,4 | -9,9 | -7,6 |
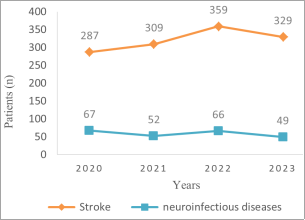
Over the course of four years, a total of 234 patients were admitted for neuroinfectious diseases, which constituted approximately 15 % of all hospital ad-missions. Within this group, brain abscesses emerged as the predominant condition, with 127 instances recorded, representing 53.6% of the cases. It is noteworthy that there was an average annual decline of 7.6% in the incidence of neuroinfectious diseases throughout this timeframe.
Figure 2. Trend in strokes versus neuroinfectious diseases Admissions (N= 1518).
3.5. Trend in In-Hospital Mortality Associated with Stroke and Neuroinfectious Diseases
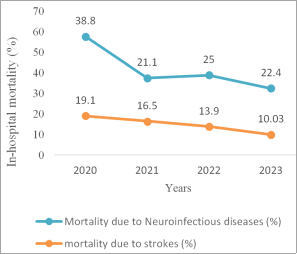
In patients hospitalized due to stroke and neuroinfectious diseases, the observed mortality rates are 15.1% and 28%, respectively. Within the category of ischemic strokes, the case-fatality rate is approximately 18.6%, whereas hemorrhagic strokes exhibit a lower case-fatality rate of 10.1%. In the context of neuroinfectious diseases, the mortality rate associated with meningoencephalitis is notably high, reaching 40% throughout the duration of the study.
Over the course of the study, a significant reduction in mortality was recorded in both categories of diseases, with an average annual decline of approximately 3% for strokes and about 5% for infectious diseases. However, the decline manifests differently for each category: it is marked by a consistent, rapid, and linear decrease in stroke cases, while neuroinfectious diseases exhibit a slower and more fluctuating decline throughout the four years.
Figure 3. Trend in Mortality Associated with Strokes and Neuroinfectious Diseases.
Table 4. A multi variate analysis of the variables associated with the risk of mortality.
Variables | Odds-Ratio | P | Coefficient |
Intercept | 0.107 [0.0596; 0.176] | < 0.001 | -2.23 |
Neuroinfectious diseases | 2.51 [1.70; 3.69] | < 0.001 | 0.920 |
Age (+10) | 1.10 [1.01; 1.20] | 0.042 | 0.0908 |
Strokes | 0.399 [0.271; 0.590] | <0.001 | 0.9202 |
Gender | 0.9000 [0.683; 1.18] | 0.45 | -0.106 |
History of HIV | 0.107 [0.546; 0.189] | 0.92 | 0.920 |
The results of the logistic regression analysis indicated that the variables significantly associated with mortality risk include the diagnosis of a neuroinfectious disease (OR = 2.50; p < 0.001) and the patient's older age (OR = 1.1; p = 0.043). Conversely, a diagnosis of stroke was associated with a reduced risk of mortality (OR = 0.39; p < 0.001). Additionally, a history of prior HIV infection did not show a correlation with a risk of death.
4. Discussion
This research highlights the variations in admission and mortality rates associated with strokes and neuroinfectious diseases. It is based on a retrospective analysis conducted over a four-year period within a neurology department of a tertiary hospital located in a tropical region. Previous studies in similar contexts, characterized by limited resources and challenges in accessing care for populations affected by cerebrovascular diseases, particularly strokes, as well as the re-emergence of central nervous system infections, are relatively scarce. Furthermore, the lack of large-scale registries and the difficulties in conducting community surveys render hospital-based studies the most relevant source of information in our area.
The findings of this study revealed that Strokes were the leading cause of admissions in our department, constituting 69% of the total cases. We recorded an average annual rise of 2% in stroke-related admissions. Nevertheless, throughout the study period, the mortality rate associated with strokes demonstrated an annual reduction of roughly 3.7%. Regarding neuroinfectious diseases, they made up 15% of the study population, and we observed a significant decline in their admission rate, with an annual reduction of approximately 7.6%. In contrast, the mortality rate for neuroinfectious diseases is alarmingly high, reaching about 28%, compared to a 15% mortality rate for strokes during our study period. Additionally, a diagnosis of a neuroinfectious disease considerably increases the risk of mortality within the hospital setting.
Our findings indicated a consistent linear rise in the incidence of stroke cases, with an estimated annual growth rate of 2%.
The investigation demonstrated that ischemic strokes, comprising 725 cases (56.7%), were more prevalent than hemorrhagic strokes, which accounted for 559 cases (43.2%). Notably, the frequency of ischemic strokes has declined by roughly 3.76%, whereas hemorrhagic strokes have experienced an average annual increase of approximately 5.2%.
Historically, strokes were rarely reported in Africa throughout the previous century
. However, by the early 2000s, our department observed a notable shift, as strokes became the second most prevalent cause of hospital admissions, comprising 43.6% of cases, while infectious diseases accounted for 46.8%
. Currently, strokes have emerged as the leading cause of hospitalization.
The 2019 Global Stroke Statistics Update revealed a consistent rise in stroke incidence across low- and middle-income nations, based on studies conducted from 1971 to 2024
. Several hospitals in Africa have documented a gradual increase in stroke admissions over the years. For example, in Tanzania, the stroke admission rate increased from 23 per 100,000 individuals in 1935 to 86 per 100,000 in 1962. Likewise, in Ghana, annual hospitalizations for stroke surged from approximately 50 in 1960 to 622 in 1993, with the percentage of total adult medical admissions due to stroke rising from under 2% in 1960 to about 12% in 1993
.
Table 5.
Epidemiological studies conducted within our neurology department from 1998 to 2023 , 15, 16]. Characteristics and outcomes of studies | Cowppli-Bony Et al. ** | Évelyne Aka-Anghui Diarra Et al.*** | Evelyne Aka- Anghui Diarra Et al.**** | [16] | Evelyne A, Zakaria M, Mohamed S, Berthe A. Profil épidémiologique et étiologique des méningo-encéphalites infectieuses observées dans le service de neurologie du CHU de Cocody (Abidjan). Revue Neurologique. 2015 ; 171 : A137. https://doi.org/10.1016/j.neurol.2015.01.297 |
[16] | Chubaka Et al. (This survey) |
Study period | 1998-2000 | 2009-2013 | 2013 | 2020-2023 |
Study population | 1018 | NA* | 189 | 1518 |
HIV-positive patients (%) | 21,9 | NA | 16,8 | 8 |
Stroke admission frequency (%) | 43,6 | 52 | NA | 69 |
Neuroinfectious diseases admission Frequency (%) | 46,8 | NA | 25,7 | 13 |
Mortality due to stroke (%) | 30,5 | 24 | NA | 15 |
Mortality due to neuroinfectious diseases (%) | 28,3 | NA | NA | 28 |
** The study included all patients admitted to the neurology department.
***The study included only stroke patients
**** The study included only patients admitted for neuroinfectious diseases
The most extensive research, carried out in Tanzania and published in 2010, indicated age-adjusted incidence rates of 109 per 100,000 person-years in rural Hai and 316 per 100,000 person-years in urban Dar es Salaam
.
The increase in cerebrovascular disease, is attributed to a combination of factors. Improved living conditions and factors specific to tropical environments, such as undernutrition in utero and early in life, contribute to this trend. These conditions are associated with an increase in cardiovascular risk factors in mid-life
. Other contributing factors include increased exposure to fine-particle air pollution, alcohol and drug abuse, and the effects of industrialization and urbanization
| [20] | Azarpazhooh MR, Hachinski V. Air pollution: A silent common killer for stroke and dementia. Int J Stroke. 2018; 13(7): 667-668. https://doi.org/10.1177/1747493018784476 |
| [21] | Wichmann J, Voyi K. Ambient air pollution exposure and respiratory, cardiovascular and cerebrovascular mortality in Cape Town, South Africa: 2001–2006. Int J Environ Res Public Health. 2012; 9(11): 3978-4016. https://doi.org/10.3390/ijerph9113978 |
[20, 21]
. Changing dietary habits and an ageing population also play a significant role
. According to WHO, by 2030, almost 80% of strokes will occur in low- and middle-income countries
. This highlights the global health challenge posed by strokes and the need for comprehensive strategies to prevent and manage them, particularly in resource-limited settings.
NCDs are identified by the WHO as one of the foremost challenges to health and development in the 21st century. These diseases not only inflict significant human suffering but also adversely impact the socio-economic frameworks of nations, particularly those classified as low and middle income
| [25] | Bennett JE, Stevens GA, Mathers CD, et al. NCD Countdown 2030: worldwide trends in non-communicable disease mortality and progress towards Sustainable Development Goal target 3.4. The Lancet. 2018; 392(10152): 1072-1088. https://doi.org/10.1016/S0140-6736(18)31992-5 |
| [26] | Bigna JJ, Noubiap JJ. The rising burden of non-communicable diseases in sub-Saharan Africa. The Lancet Global Health. 2019; 7(10): e1295-e1296. https://doi.org/10.1016/S2214-109X(19)30370-5 |
[25, 26]
. The increasing prevalence of NCDs represents a critical issue that demands the attention of all governments. Each year, NCDs account for the premature deaths of 17 million individuals under the age of 70, with an alarming 86% of these fatalities occurring in low and middle-income countries.
Among these, cardiovascular diseases, including strokes, are the leading cause of NCD-related deaths, contributing to a total of 17.9 million fatalities annually
| [13] | Kim J, Thayabaranathan T, Donnan GA, et al. Global Stroke Statistics 2019. Int J Stroke. 2020; 15(8): 819-838. https://doi.org/10.1177/1747493020909545 |
| [25] | Bennett JE, Stevens GA, Mathers CD, et al. NCD Countdown 2030: worldwide trends in non-communicable disease mortality and progress towards Sustainable Development Goal target 3.4. The Lancet. 2018; 392(10152): 1072-1088. https://doi.org/10.1016/S0140-6736(18)31992-5 |
[13, 25]
.
A decade ago, the WHO introduced a comprehensive strategy comprising nine ambitious objectives to be realized by the year 2025. Among these objectives were a 25% reduction in mortality rates associated with cardiovascular diseases, a 10% decrease in the prevalence of physical inactivity and harmful alcohol consumption, a 30% reduction in average salt intake across the population, and a 30% decline in smoking rates among individuals aged 15 and older. The strategy also aimed for a 25% reduction or stabilization in hypertension prevalence, contingent upon national circumstances, alongside a cessation of the upward trends in diabetes and obesity. Additionally, it sought to ensure that at least 50% of eligible individuals receive preventive chemotherapy and counseling, including measures for blood sugar management, to avert heart attacks and strokes. Finally, the plan aimed to guarantee that 80% of essential medications, including generics, and critical technologies for managing major non-communicable diseases are both financially accessible and available in public and private healthcare facilities
. As the year 2025 draws near, it is clear that health policies regarding stroke screening and prevention require further enhancement, particularly in tropical regions. Noteworthy advancements have been observed in certain African nations, such as Rwanda, which has implemented the ‘Kigali Car Free Day’ initiative
| [28] | Kabakambira JD, Bitwayiki RN, Mujawamariya G, Lucero-Prisno III DE& M. Kigali Car Free Day: An Innovative Model in the Fight against Non-Communicable Disease Pandemics. Rwanda Medical Journal. 76(3): 1-5. |
| [29] | Glazener A, Wylie J, van Waas W, Khreis H. The Impacts of Car-Free Days and Events on the Environment and Human Health. Curr Envir Health Rpt. 2022; 9(2): 165-182. https://doi.org/10.1007/s40572-022-00342-y |
[28, 29]
, an innovative approach that integrates the combat against non-communicable diseases with environmental sustainability, providing free screenings for cardiovascular risk factors.
Our research indicated that the in-hospital mortality rate linked to strokes was determined to be 15%. Additionally, the investigation recorded case-fatality rates of approximately 18.6% for ischemic strokes and 10.1% for hemorrhagic strokes. Comparative data suggests that stroke mortality rates in certain regions of Africa may be higher than global averages. For instance, the INTERSTROKE hospital study reported a one-month stroke case-fatality rate of 22% in Africa, significantly higher than the 4% observed in high-income countries
| [30] | O’Donnell MJ, Chin SL, Rangarajan S, et al. Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): a case-control study. Lancet. 2016; 388(10046): 761-775. https://doi.org/10.1016/S0140-6736(16)30506-2 |
[30]
. Additional hospital research performed in Africa has demonstrated a considerable disparity in 30-day mortality rates, spanning from 16.2% to a striking 46%
| [4] | Maredza M, Bertram MY, Tollman SM. Disease burden of stroke in rural South Africa: an estimate of incidence, mortality and disability adjusted life years. BMC Neurol. 2015; 15: 54. https://doi.org/10.1186/s12883-015-0311-7 |
[4]
,
| [5] | Lekoubou A, Nkoke C, Dzudie A, Kengne AP. Stroke admission and case-fatality in an urban medical unit in sub-Saharan Africa: a fourteen year trend study from 1999 to 2012. J Neurol Sci. 2015; 350(1-2): 24-32. https://doi.org/10.1016/j.jns.2015.02.002 |
[5]
. A detailed review and meta-analysis concerning stroke mortality in sub-Saharan Africa, published in 2021, found a one-month mortality rate of 24.1%
| [31] | Okekunle AP, Jones S, Adeniji O, et al. Stroke in Africa: A systematic review and meta-analysis of the incidence and case-fatality rates. Int J Stroke. 2023; 18(6): 634-644. https://doi.org/10.1177/17474930221147164 |
[31]
. This rate, however, was marked by considerable variation, with certain regions experiencing rates as high as 83.3%
| [31] | Okekunle AP, Jones S, Adeniji O, et al. Stroke in Africa: A systematic review and meta-analysis of the incidence and case-fatality rates. Int J Stroke. 2023; 18(6): 634-644. https://doi.org/10.1177/17474930221147164 |
[31]
.
According to the data presented in
Table 5, which depicts the findings from epidemiological studies conducted in our neurology department from 1998 to 2023, it is clear that there has been a significant decline in mortality rates associated with strokes. Over the span of 25 years, this rate has decreased from nearly 30% in 1998 to just 15% in 2023, indicating a reduction of approximately 50%. The decline in stroke mortality noted in our study can be attributed to better access to healthcare services and the utilization of advanced imaging technologies such as brain CT and MRI, which allow for faster diagnostic processes. Additionally, the growing number of qualified healthcare professionals has led to improved care during the acute phase and more effective management of cardiovascular and metabolic risk factors, including hypertension, diabetes, and heart conditions. These developments in acute care have significantly affected the prognosis of hemorrhagic strokes. Nonetheless, the complications that arise from prolonged bed rest, particularly infections, may contribute to the increased mortality rates associated with ischemic strokes, which are often linked to severe disability from the outset. While improvements in acute management have been essential in reducing stroke mortality, it remains vital to prioritize prevention and the management of decubitus complications to further enhance patient outcomes
| [32] | Seminog OO, Scarborough P, Wright FL, Rayner M, Goldacre MJ. Determinants of the decline in mortality from acute stroke in England: linked national database study of 795 869 adults. BMJ. 2019; 365: l1778. https://doi.org/10.1136/bmj.l1778 |
[32]
.
Over the study period, neuro-infectious diseases constituted approximately 13% of the overall admissions recorded. During the year 2000, they were the leading cause of admissions in neurology, making up roughly 46.8% of all cases
. From 2000 to 2023, this prevalence has diminished by approximately 72%, and they now rank as the second most prevalent cause of admissions in the same department. The reduction in the frequency of neuroinfectious diseases can be primarily attributed to the decline in both the incidence and prevalence of HIV within the population, as well as the adherence to treatment among individuals living with HIV
| [16] | Evelyne A, Zakaria M, Mohamed S, Berthe A. Profil épidémiologique et étiologique des méningo-encéphalites infectieuses observées dans le service de neurologie du CHU de Cocody (Abidjan). Revue Neurologique. 2015 ; 171 : A137. https://doi.org/10.1016/j.neurol.2015.01.297 |
[16]
. Indeed, the majority of neuroinfectious diseases occur in immunocompromised individuals. In the year 2000, within the neurology department of COCODY in Abidjan, HIV-immunocompromised patients accounted for 21.9% of cases
, whereas this figure decreased to 16.8% in 2013
| [16] | Evelyne A, Zakaria M, Mohamed S, Berthe A. Profil épidémiologique et étiologique des méningo-encéphalites infectieuses observées dans le service de neurologie du CHU de Cocody (Abidjan). Revue Neurologique. 2015 ; 171 : A137. https://doi.org/10.1016/j.neurol.2015.01.297 |
[16]
, and it currently stands at a mere 8%.
Although our study indicates a decrease in annual mortality associated with neuro-infectious diseases (around 17% per year), the overall mortality rate linked to these diseases over the four-year observation period remains virtually unchanged compared to the rate recorded 25 years ago by Cowppli-Bony et al. in 2000
, which was approximately 28%. The diagnosis of a neuro-infectious disease is associated with an increased risk of mortality, with an odds ratio (OR) of 2.51 [1.70; 3.69], p < 0.001, while strokes present an OR of 0.399 [0.271; 0.590], p < 0.001. The ongoing prevalence of mortality rates associated with neuroinfectious diseases can be largely attributed to the healthcare journey of patients in Africa. This journey is frequently marked by delays in seeking medical consultation, often preceded by the use of traditional treatments
| [33] | Ouendo EM, Makoutodé M, Paraiso MN, Wilmet-Dramaix M, Dujardin B. Itinéraire thérapeutique des malades indigents au Bénin (Pauvreté et soins de santé). Tropical Medicine & International Health. 2005; 10(2): 179-186. https://doi.org/10.1111/j.1365-3156.2004.01371.x |
[33]
, as well as diagnostic misdirection within small community healthcare facilities. Such factors significantly hinder timely access to appropriate medical care. Consequently, patients often arrive at our facility in a state of advanced sepsis, which severely jeopardizes their prognosis.
It is undeniable that the "Western world" has undergone a significant transformation, evolving from a state of underdevelopment to one of development, which has resulted in a notable decrease in mortality rates associated with infectious diseases. However, this progress has not been evenly distributed, particularly in the Global South, where developmental delays pose a major challenge
| [34] | Caselli G. The key phases of the European health transition. Pol Popul Rev. 1995; (7): 73-102. |
| [35] | Frenk J, Bobadilla JL, Stern C, Frejka T, Lozano R. Elements for a theory of the health transition. Health Transit Rev. 1991; 1(1): 21-38. |
| [36] | Olshansky SJ, Ault AB. The fourth stage of the epidemiologic transition: the age of delayed degenerative diseases. Milbank Q. 1986; 64(3): 355-391. |
[34-36]
. This inequality has sparked ongoing debates and concerns regarding the applicability of the Western health development model in tropical regions. Fifty years ago, there was considerable optimism due to advancements in the fight against infectious diseases, attributed to improvements in hygiene, environmental health, the introduction of antibiotics, vaccination campaigns, and broader social progress
| [10] | Desenclos JC, De Valk H. [Emergent infectious diseases: importance for public health, epidemiology, promoting factors, and prevention]. Med Mal Infect. 2005; 35(2): 49-61. https://doi.org/10.1016/j.medmal.2004.09.005 |
[10]
. Nevertheless, contemporary public health officials cannot overlook the challenges posed by infectious diseases. The emergence of the Coronavirus pandemic in 2019 highlighted the reality of emerging and re-emerging infections, underscoring their ability to spread rapidly on a global scale
| [36] | Olshansky SJ, Ault AB. The fourth stage of the epidemiologic transition: the age of delayed degenerative diseases. Milbank Q. 1986; 64(3): 355-391. |
[36]
. It is also important to note that many of these re-emerging diseases lead to neurological complications during the acute phase, while other neurological manifestations may appear later
| [37] | Berkowitz AL, Raibagkar P, Pritt BS, Mateen FJ. Neurologic manifestations of the neglected tropical diseases. Journal of the Neurological Sciences. 2015; 349(1): 20-32. https://doi.org/10.1016/j.jns.2015.01.001 |
[37]
.
These findings raise significant concerns among various health stakeholders, particularly neurologists and public health policymakers. In an era that appears to prioritize neurovascular emergencies, it is crucial to establish an appropriate health policy for neuro-infectious emergencies. This policy should involve a range of healthcare professionals, especially those working in community health centers, who frequently serve as the initial point of contact for patients. It is vital that these professionals receive training to identify the signs of cerebral and meningeal infections, thereby facilitating early diagnosis and referral to suitable healthcare facilities.
Neurologists in Africa, particularly in Ivory Coast, encounter a range of complex and interconnected challenges. They are faced with the increasing prevalence of non-communicable diseases, especially neurovascular conditions such as strokes, while simultaneously addressing persistent infections with neurological manifestations, including HIV and tuberculosis, which can also lead to strokes, thereby creating a vicious cycle. These issues are further complicated by factors such as overcrowding, within a context of demographic shifts and an ever-changing environment, as well as a shortage of specialized professionals and diagnostic tools. To effectively tackle these challenges and enhance the management of both disease categories, it is essential to conduct large-scale prospective analytical studies involving multiple centers. This approach will deepen our understanding of the underlying factors driving these epidemiological trends and provide context-specific data, thereby facilitating improvements in medical practices and health policies across African nations, ultimately aiming to alleviate the burdens associated with these two groups of diseases.
5. Conclusions
This research highlights an increase in admissions related to cerebrovascular accidents, while a decrease is noted for neuroinfectious diseases. Nevertheless, the latter continue to pose a significant burden in terms of in-hospital mortality, particularly among young adults. To address these challenges, it is essential to enhance health policies concerning both types of conditions. This improvement necessitates a strengthening of cardiovascular risk assessment and prevention strategies, as well as the allocation of adequate resources and personnel for the acute management of strokes and the prevention of complications associated with immobilization, which contribute to in-hospital mortality.
Furthermore, it is crucial to develop guidelines tailored to tropical contexts and to educate both the public and primary healthcare professionals about the early signs of infectious diseases affecting the brain, ensuring timely referral of patients to specialized medical facilities. Community-based research should also be conducted to better understand the factors contributing to delays in consultation among patients with neuroinfectious diseases, as well as those related to dietary habit changes in Africa.
Abbreviations
NCDs | Non Communicable Diseases |
WHO | World Health Organization |
DALYs | Disability-Adjusted Life Years |
CSF | Cerebrospinal Fluid |
NA | Not Attributed |
HIV | Human Immunodeficiency Virus |
OD | Odds Ratio |
CT | Computed Tomography |
MRI | Magnetic Resonance Imaging |
Acknowledgments
The lead author, Gloire Chubaka Magala, expresses profound gratitude to the entire committee of the BEBUC Excellence Scholarship Program for their steadfast confidence, encouragements and financial assistance rendered throughout his master's studies in clinical neuroscience.
Author Contributions
Gloire Chubaka Magala: Conceptualization, formal analysis, Funding acquisition, writing the original draft
Muriel Amon-Tanoh: Funding acquisition, Methodology
Abel Christian Tanoh: Funding acquisition, Project administration
Cédric Valéry Kadjo: Investigation, Project administration, Resources, Software, Validation, Visualization
Jonathan Bachiseze Magala: Investigation, Project administration, Resources, Software, Validation, Visualization
Fiacre Delors Offoumou: Investigation, Project administration, Resources, Software, Validation, Visualization
Désirée Aka Arlette: Investigation, Project administration, Resources, Software, Validation, Visualization
Constance Yapo-Ehounoud: Investigation, Project administration, Resources, Software, Validation, Visualization
Nancy Tania Essoin-De Souza: Investigation, Project administration, Resources, Software, Validation, Visualization
Yves Broh N’guessan: Investigation, Project administration, Resources, Software, Validation, Visualization
Mavouloh Kourouma: Investigation, Project administration, Resources, Software, Validation, Visualization
Évelyne Aka-Anghui Diarra: Supervision, Validation
Berthe Assi: Investigation, Project administration, Resources, Software, Validation, Visualization
Funding
The authors did not receive any funding for this study.
Data Availability Statement
The database used and analyzed during the current study is available from the corresponding author and will available on request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Wahdan MH. The epidemiological transition. EMHJ - Eastern Mediterranean Health Journal, 2 (1), 8-20, 1996. Published online 1996. Accessed August 25, 2024.
https://iris.who.int/handle/10665/118829
|
| [2] |
GBD 2019 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021; 20(10): 795-820.
https://doi.org/10.1016/S1474-4422(21)00252-0
|
| [3] |
Walker R, Whiting D, Unwin N, et al. Stroke incidence in rural and urban Tanzania: a prospective, community-based study. Lancet Neurol. 2010; 9(8): 786-792.
https://doi.org/10.1016/S1474-4422(10)70144-7
|
| [4] |
Maredza M, Bertram MY, Tollman SM. Disease burden of stroke in rural South Africa: an estimate of incidence, mortality and disability adjusted life years. BMC Neurol. 2015; 15: 54.
https://doi.org/10.1186/s12883-015-0311-7
|
| [5] |
Lekoubou A, Nkoke C, Dzudie A, Kengne AP. Stroke admission and case-fatality in an urban medical unit in sub-Saharan Africa: a fourteen year trend study from 1999 to 2012. J Neurol Sci. 2015; 350(1-2): 24-32.
https://doi.org/10.1016/j.jns.2015.02.002
|
| [6] |
Feigin VL, Vos T, Nichols E, et al. The global burden of neurological disorders: translating evidence into policy. Lancet Neurol. 2020; 19(3): 255-265.
https://doi.org/10.1016/S1474-4422(19)30411-9
|
| [7] |
Rocklöv J, Dubrow R. Climate change: an enduring challenge for vector-borne disease prevention and control. Nat Immunol. 2020; 21(5): 479-483.
https://doi.org/10.1038/s41590-020-0648-y
|
| [8] |
Wahab KW. The burden of stroke in Nigeria. Int J Stroke. 2008; 3(4): 290-292.
https://doi.org/10.1111/j.1747-4949.2008.00217.x
|
| [9] |
Institute of Medicine (US) Committee on Emerging Microbial Threats to Health in the 21st Century. Microbial Threats to Health: Emergence, Detection, and Response. (Smolinski MS, Hamburg MA, Lederberg J, eds.). National Academies Press (US); 2003. Accessed August 25, 2024.
http://www.ncbi.nlm.nih.gov/books/NBK221486/
|
| [10] |
Desenclos JC, De Valk H. [Emergent infectious diseases: importance for public health, epidemiology, promoting factors, and prevention]. Med Mal Infect. 2005; 35(2): 49-61.
https://doi.org/10.1016/j.medmal.2004.09.005
|
| [11] |
Cowppli B, Sonan T, Akani F, Datie A. [Epidemiologie des patients hospitalisés en neurologie: experience du centre hospitalier universitaire de cocody à abidjan]. AJNS. [AJNS 2004 Vol. 23, No 2] Accessed March 27, 2024.
https://ajns.paans.org/epidemiologie-des-patients-hospitalises-en-neurologie-experience-du-centre-hospitalier-universitaire-de-cocody-a-abidjan-cote-divoire/
|
| [12] |
B O Osuntokun, Stroke in the Africans. Afr J Med Med Sci 1977 Jun; 6(2): 39-53. Accessed August 25, 2024.
https://pubmed.ncbi.nlm.nih.gov/416666/
|
| [13] |
Kim J, Thayabaranathan T, Donnan GA, et al. Global Stroke Statistics 2019. Int J Stroke. 2020; 15(8): 819-838.
https://doi.org/10.1177/1747493020909545
|
| [14] |
Connor MD, Walker R, Modi G, Warlow CP. Burden of stroke in black populations in sub-Saharan Africa. Lancet Neurol. 2007; 6(3): 269-278.
https://doi.org/10.1016/S1474-4422(07)70002-9
|
| [15] |
Diarra ÉAA, Assouan AEK, Yao RB, Kouame LK, Kadjo C, Tanoh C. Épidémiologie des AVC en Côte d’Ivoire et perspectives. Revue Neurologique. 2016; 172: A164.
https://doi.org/10.1016/j.neurol.2016.01.391
|
| [16] |
Evelyne A, Zakaria M, Mohamed S, Berthe A. Profil épidémiologique et étiologique des méningo-encéphalites infectieuses observées dans le service de neurologie du CHU de Cocody (Abidjan). Revue Neurologique. 2015 ; 171 : A137.
https://doi.org/10.1016/j.neurol.2015.01.297
|
| [17] |
Barker DJ. The intrauterine origins of cardiovascular disease. Acta Paediatr Suppl. 1993; 82 Suppl 391: 93-99; discussion 100.
https://doi.org/10.1111/j.1651-2227.1993.tb12938.x
|
| [18] |
D J Barker. The intrauterine environment and adult cardiovascular disease. Ciba Found Symp. 1991: 156: 3-10.
https://doi.org/10.1002/9780470514047.ch2
|
| [19] |
Hult M, Tornhammar P, Ueda P, et al. Hypertension, diabetes and overweight: looming legacies of the Biafran famine. PLoS One. 2010; 5(10): e13582.
https://doi.org/10.1371/journal.pone.0013582
|
| [20] |
Azarpazhooh MR, Hachinski V. Air pollution: A silent common killer for stroke and dementia. Int J Stroke. 2018; 13(7): 667-668.
https://doi.org/10.1177/1747493018784476
|
| [21] |
Wichmann J, Voyi K. Ambient air pollution exposure and respiratory, cardiovascular and cerebrovascular mortality in Cape Town, South Africa: 2001–2006. Int J Environ Res Public Health. 2012; 9(11): 3978-4016.
https://doi.org/10.3390/ijerph9113978
|
| [22] |
Keates AK, Mocumbi AO, Ntsekhe M, Sliwa K, Stewart S. Cardiovascular disease in Africa: epidemiological profile and challenges. Nat Rev Cardiol. 2017; 14(5): 273-293.
https://doi.org/10.1038/nrcardio.2017.19
|
| [23] |
Knowledge of risk among patients at increased risk for stroke - PubMed. Accessed August 25, 2024.
https://pubmed.ncbi.nlm.nih.gov/9158625/
|
| [24] |
Akinyemi RO, Owolabi MO, Ihara M, et al. Stroke, cerebrovascular diseases and vascular cognitive impairment in Africa. Brain Res Bull. 2019; 145: 97-108.
https://doi.org/10.1016/j.brainresbull.2018.05.018
|
| [25] |
Bennett JE, Stevens GA, Mathers CD, et al. NCD Countdown 2030: worldwide trends in non-communicable disease mortality and progress towards Sustainable Development Goal target 3.4. The Lancet. 2018; 392(10152): 1072-1088.
https://doi.org/10.1016/S0140-6736(18)31992-5
|
| [26] |
Bigna JJ, Noubiap JJ. The rising burden of non-communicable diseases in sub-Saharan Africa. The Lancet Global Health. 2019; 7(10): e1295-e1296.
https://doi.org/10.1016/S2214-109X(19)30370-5
|
| [27] |
Maladies non transmissibles. Accessed August 25, 2024.
https://www.who.int/fr/news-room/fact-sheets/detail/noncommunicable-diseases
|
| [28] |
Kabakambira JD, Bitwayiki RN, Mujawamariya G, Lucero-Prisno III DE& M. Kigali Car Free Day: An Innovative Model in the Fight against Non-Communicable Disease Pandemics. Rwanda Medical Journal. 76(3): 1-5.
|
| [29] |
Glazener A, Wylie J, van Waas W, Khreis H. The Impacts of Car-Free Days and Events on the Environment and Human Health. Curr Envir Health Rpt. 2022; 9(2): 165-182.
https://doi.org/10.1007/s40572-022-00342-y
|
| [30] |
O’Donnell MJ, Chin SL, Rangarajan S, et al. Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): a case-control study. Lancet. 2016; 388(10046): 761-775.
https://doi.org/10.1016/S0140-6736(16)30506-2
|
| [31] |
Okekunle AP, Jones S, Adeniji O, et al. Stroke in Africa: A systematic review and meta-analysis of the incidence and case-fatality rates. Int J Stroke. 2023; 18(6): 634-644.
https://doi.org/10.1177/17474930221147164
|
| [32] |
Seminog OO, Scarborough P, Wright FL, Rayner M, Goldacre MJ. Determinants of the decline in mortality from acute stroke in England: linked national database study of 795 869 adults. BMJ. 2019; 365: l1778.
https://doi.org/10.1136/bmj.l1778
|
| [33] |
Ouendo EM, Makoutodé M, Paraiso MN, Wilmet-Dramaix M, Dujardin B. Itinéraire thérapeutique des malades indigents au Bénin (Pauvreté et soins de santé). Tropical Medicine & International Health. 2005; 10(2): 179-186.
https://doi.org/10.1111/j.1365-3156.2004.01371.x
|
| [34] |
Caselli G. The key phases of the European health transition. Pol Popul Rev. 1995; (7): 73-102.
|
| [35] |
Frenk J, Bobadilla JL, Stern C, Frejka T, Lozano R. Elements for a theory of the health transition. Health Transit Rev. 1991; 1(1): 21-38.
|
| [36] |
Olshansky SJ, Ault AB. The fourth stage of the epidemiologic transition: the age of delayed degenerative diseases. Milbank Q. 1986; 64(3): 355-391.
|
| [37] |
Berkowitz AL, Raibagkar P, Pritt BS, Mateen FJ. Neurologic manifestations of the neglected tropical diseases. Journal of the Neurological Sciences. 2015; 349(1): 20-32.
https://doi.org/10.1016/j.jns.2015.01.001
|
Cite This Article
-
APA Style
Magala, G. C., Tanoh, M. A., Tanoh, A. C., Kadjo, C. V., Magala, J. B., et al. (2024). Epidemiological Trends Related to Stroke and Neuroinfectious Diseases in Patients Admitted to the Neurology Unit at Cocody Teaching Hospital in Abidjan. European Journal of Preventive Medicine, 12(5), 121-131. https://doi.org/10.11648/j.ejpm.20241205.12
 Copy
|
Copy
|
 Download
Download
ACS Style
Magala, G. C.; Tanoh, M. A.; Tanoh, A. C.; Kadjo, C. V.; Magala, J. B., et al. Epidemiological Trends Related to Stroke and Neuroinfectious Diseases in Patients Admitted to the Neurology Unit at Cocody Teaching Hospital in Abidjan. Eur. J. Prev. Med. 2024, 12(5), 121-131. doi: 10.11648/j.ejpm.20241205.12
Copy
|
Download
AMA Style
Magala GC, Tanoh MA, Tanoh AC, Kadjo CV, Magala JB, et al. Epidemiological Trends Related to Stroke and Neuroinfectious Diseases in Patients Admitted to the Neurology Unit at Cocody Teaching Hospital in Abidjan. Eur J Prev Med. 2024;12(5):121-131. doi: 10.11648/j.ejpm.20241205.12
Copy
|
Download
-
@article{10.11648/j.ejpm.20241205.12,
author = {Gloire Chubaka Magala and Muriel Amon Tanoh and Abel Christian Tanoh and Cedric Valery Kadjo and Jonathan Bachiseze Magala and Fiacre Delors Offoumou and Desirée Aka Arlette and Constance Yapo Ehounoud and Nancy Tania Essoin-De Souza and Yves Broh N’guessan and Mavouloh Kourouma and Evelyne Aka-Anghui Diarra and Berthe Assi},
title = {Epidemiological Trends Related to Stroke and Neuroinfectious Diseases in Patients Admitted to the Neurology Unit at Cocody Teaching Hospital in Abidjan
},
journal = {European Journal of Preventive Medicine},
volume = {12},
number = {5},
pages = {121-131},
doi = {10.11648/j.ejpm.20241205.12},
url = {https://doi.org/10.11648/j.ejpm.20241205.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ejpm.20241205.12},
abstract = {Background: In Ivory Coast, as in many tropical regions, there is a significant coexistence of infectious diseases and non-communicable diseases (NCDs), particularly within the field of neurology. The dual burden of neuroinfectious diseases, including meningitis and strokes, plays a crucial role in shaping public health strategies implemented by the World Health Organization (WHO) and national health programs. Unfortunately, the epidemiological trends are not regularly updated. This study aims to provide insights into hospital admissions and mortality related to strokes and brain infections to inform health policies and improve disease management. Method: It was a retrospective study that examined the medical records of patients admitted to the neurology department of the Cocody University Hospital in Abidjan from January 1, 2020, to December 31, 2023, and included individuals across all age groups who were diagnosed with stroke, brain abscess, meningitis, or encephalitis. Results: The study involved 1,518 patients, strokes were more common among older adults, with an average age of 57.3 ± 13.7 years. Strokes represented the primary reason for hospitalization, making up 69% of cases, with an annual growth rate of approximately 2%, while neuroinfectious diseases accounted for 13% of total admissions. In-hospital mortality rates were 15% for stroke patients and 28% for those with neuroinfectious diseases, the latter showing a significantly higher mortality risk (odds ratio = 2.50; p < 0.001). Conclusion: Strokes are the leading cause of hospital admissions in our department, with increasing rates; however, neuroinfectious diseases have higher and stable mortality rates, indicating a more severe prognosis. Therefore, health policies must be reassessed to improve prevention and management for both diseases.
},
year = {2024}
}
Copy
|
Download
-
TY - JOUR
T1 - Epidemiological Trends Related to Stroke and Neuroinfectious Diseases in Patients Admitted to the Neurology Unit at Cocody Teaching Hospital in Abidjan
AU - Gloire Chubaka Magala
AU - Muriel Amon Tanoh
AU - Abel Christian Tanoh
AU - Cedric Valery Kadjo
AU - Jonathan Bachiseze Magala
AU - Fiacre Delors Offoumou
AU - Desirée Aka Arlette
AU - Constance Yapo Ehounoud
AU - Nancy Tania Essoin-De Souza
AU - Yves Broh N’guessan
AU - Mavouloh Kourouma
AU - Evelyne Aka-Anghui Diarra
AU - Berthe Assi
Y1 - 2024/09/29
PY - 2024
N1 - https://doi.org/10.11648/j.ejpm.20241205.12
DO - 10.11648/j.ejpm.20241205.12
T2 - European Journal of Preventive Medicine
JF - European Journal of Preventive Medicine
JO - European Journal of Preventive Medicine
SP - 121
EP - 131
PB - Science Publishing Group
SN - 2330-8230
UR - https://doi.org/10.11648/j.ejpm.20241205.12
AB - Background: In Ivory Coast, as in many tropical regions, there is a significant coexistence of infectious diseases and non-communicable diseases (NCDs), particularly within the field of neurology. The dual burden of neuroinfectious diseases, including meningitis and strokes, plays a crucial role in shaping public health strategies implemented by the World Health Organization (WHO) and national health programs. Unfortunately, the epidemiological trends are not regularly updated. This study aims to provide insights into hospital admissions and mortality related to strokes and brain infections to inform health policies and improve disease management. Method: It was a retrospective study that examined the medical records of patients admitted to the neurology department of the Cocody University Hospital in Abidjan from January 1, 2020, to December 31, 2023, and included individuals across all age groups who were diagnosed with stroke, brain abscess, meningitis, or encephalitis. Results: The study involved 1,518 patients, strokes were more common among older adults, with an average age of 57.3 ± 13.7 years. Strokes represented the primary reason for hospitalization, making up 69% of cases, with an annual growth rate of approximately 2%, while neuroinfectious diseases accounted for 13% of total admissions. In-hospital mortality rates were 15% for stroke patients and 28% for those with neuroinfectious diseases, the latter showing a significantly higher mortality risk (odds ratio = 2.50; p < 0.001). Conclusion: Strokes are the leading cause of hospital admissions in our department, with increasing rates; however, neuroinfectious diseases have higher and stable mortality rates, indicating a more severe prognosis. Therefore, health policies must be reassessed to improve prevention and management for both diseases.
VL - 12
IS - 5
ER -
Copy
|
Download