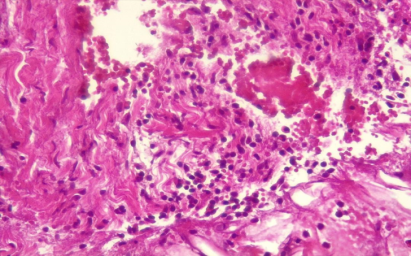
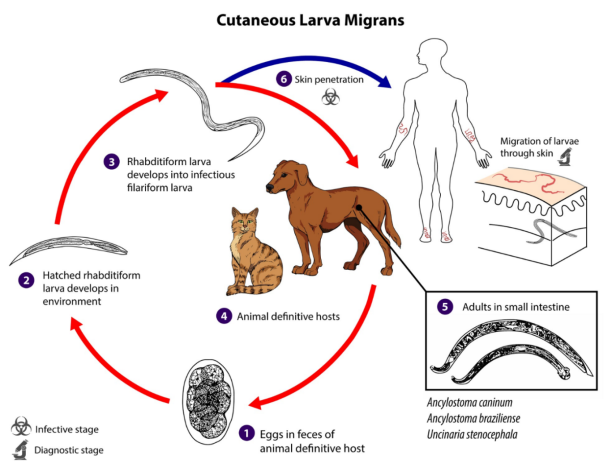
Cutaneous larva migrans is a parasitic disease typical of tropical and subtropical climate zones. In Bulgaria, cases are rare and are usually found in tourists who have visited the tropics. The disease is caused by nematode larvae, most often Ancylostoma braziliense. Humans are accidental hosts in which the larvae do not reach sexual maturity, do not complete their life cycle and die. Infection occurs through contact with contaminated soil or sand or by ingestion of nematode eggs. There are two types of larva migrans: cutaneous and visceral. The cutaneous form manifests itself with characteristic itchy, erythematous, linear or zigzag crawling lesions, while the visceral form affects internal organs such as the liver, lungs, heart and brain and is more common in children without hygiene habits. The diagnosis of the cutaneous form is based on exposure history and clinical presentation, while the visceral form requires serological tests and imaging studies. We present a 61-year-old female patient with cutaneous larva migrans acquired after travel to Zanzibar. The diagnosis was based on the typical clinical presentation, epidemiological history, and histopathological findings. Laboratory tests revealed moderate blood eosinophilia and elevated inflammatory markers. Systemic treatment with ivermectin led to rapid symptom relief and complete recovery. This case highlights the importance of early diagnosis and treatment in patients returning from endemic areas.
| Published in | International Journal of Clinical Dermatology (Volume 8, Issue 1) |
| DOI | 10.11648/j.ijcd.20250801.16 |
| Page(s) | 33-39 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Cutaneous Larva Migrans, Parasitic Infection, Tropical Regions, Eosinophilia, Ivermectin, Serpiginous Lesions, Diagnosis, Treatment
Disease | Etiology | Key Features | Localization | Migration | Systemic Symptoms | Diagnosis |
|---|---|---|---|---|---|---|
Larva currens | Strongyloides stercoralis | Linear erythematous-edematous lesions, rapid migration | Perineum, buttocks, thighs | 10 cm/day (faster than CLM) | Diarrhea, eosinophilia | Stool analysis, serology (ELISA) |
Gnathostomiasis | Gnathostoma spinigerum | Subcutaneous nodules, edema, pain | Subcutaneous tissue | Slow migration | Neurological and ocular complications | Serology, biopsy |
Fascioliasis | Fasciola hepatica, F. gigantica | Erythema, urticaria, angioedema | Various regions | None | Hepatomegaly, jaundice | Stool analysis, serology |
Filariasis | Loa loa, Onchocerca, Mansonella | Subcutaneous nodules, angioedema | Periorbital area, lymph nodes | None | Lymphadenopathy, pruritus | Blood smear microscopy, serology |
Scabies | Sarcoptes scabiei | Polymorphic lesions (papules, crusts, burrows) | Fingers, wrists, genitals | Linear burrows, not true migration | Intense nocturnal pruritus | Dermoscopy, skin scraping |
Erythema chronicum migrans | Borrelia burgdorferi | Expanding concentric erythema (“target” lesion) | Around tick bite | None | Flu-like symptoms | Serology, PCR |
Tinea cutis glabrae | Dermatophytes | Round, raised scaly lesions | Face, hands, feet | None | Itching | KOH test |
Erysipelas and Cellulitis | Streptococcus, Staphylococcus | Painful, warm, inflammatory lesions | Limbs, face | None | Fever, leukocytosis | CRP, bacterial culture |
Bullous pemphigoid | Autoimmune | Tense bullae, chronic course | Any body area | None | No contact with contaminated soil | Immunofluorescence, IgG/C3 in basement membrane |
Cutaneous Pili Migrans | Ingrown hairs | Linear or curvilinear erythematous lesions | Face, limbs | None | Itching, pain | Derm |
PBC | Peripheral Blood Smear |
| [1] | Caumes E. It’s time to distinguish hookworm-related cutaneous larva migrans from other creeping eruptions. Clin Infect Dis. 2000; 30 (5): 803–804. |
| [2] | Blackwell V, Vega-Lopez F. Cutaneous larva migrans: clinical features and management of 44 cases presenting in the returning traveler. Br J Dermatol. 2001; 145 (3): 434–437. |
| [3] | Heukelbach J, Jackson A, Ariza L, Feldmeier H. Prevalence and risk factors of hookworm-related cutaneous larva migrans in a rural community in Brazil. Ann Trop Med Parasitol. 2008; 102 (1): 53–61. |
| [4] | Hochedez P, Caumes E. Common skin infections in travelers. J Travel Med. 2008; 15 (4): 252–262. |
| [5] | Prociv P, Croese J. Human enteric infection with Ancylostoma caninum: hookworms reappraised in the light of a "new" zoonosis. Acta Trop. 1996; 62 (1): 23–44. |
| [6] | Bowman DD, Montgomery SP, Zajac AM, Eberhard ML, Kazacos KR. Hookworms of dogs and cats as agents of cutaneous larva migrans. Trends Parasitol. 2010; 26 (4): 162–167. h |
| [7] | Ghoshal L, Ghosh S, Ghosh A. Cutaneous larva migrans: Review of current literature. Trop Parasitol. 2020; 10 (2): 59–66. |
| [8] | Heukelbach J, Feldmeier H. Epidemiological and clinical characteristics of hookworm-related cutaneous larva migrans. Lancet Infect Dis. 2008; 8 (5): 302–309. |
| [9] | Боева-Бангьозова В, Попова Н. Анкилостомидози. В: Боева-Бангьозова В, Вутова К, ред. Паразитология (Местни и Тропически Паразитози). София: АРСО; 2010: 269–74. |
| [10] | Brooker S, Clements ACA, Bundy DAP. Global epidemiology, ecology and control of soil-transmitted helminth infections. Adv Parasitol. 2006; 62: 221–261. |
| [11] | Hotez PJ. The rise of neglected tropical diseases in the “new normal” climate era. PLoS Negl Trop Dis. 2020; 14(5): e0008333. |
| [12] | Krolewiecki A, et al. Human infection with Ancylostoma caninum: Possible zoonotic transmission. Am J Trop Med Hyg. 2013; 89 (1): 157–159. |
| [13] | Schuster RK. Helminths of importance for dogs in tropical and subtropical regions. Vet Parasitol. 2010; 170 (1-2): 1–18. |
| [14] | Fischer PR, et al. Common skin infections in travelers. Travel Med Infect Dis. 2003; 1 (3): 163–176. |
| [15] | Blaizot R, Goiset A, Caumes É, et al. Cutaneous Larva Migrans in Europe. Eur J Dermatol. 2017; 27: 426–429. |
| [16] | Damante, J. H., Chinellato, L. E., Oliveira, F. T. Larva Migrans in the Oral Mucosa: Report of Two Cases. Brazil Dental J. 2011; 22 (2): 166-170. |
| [17] | Guimaraes, L. C, Silva, J. H., Saad, K. Larva Migrans within Scalp Sebaceous Gland. Revista Soc Brasileira Med Tropical. 1999; 32 (2): 187-189. |
| [18] | Simon, M. W., Simon, N. P. Cutaneous Larva Migrans. Ped Emergency Care. 2003; 19 (5): 350-352. |
| [19] | Green R, Somayaji R, Chia J. Bullous cutaneous larva migrans. Can Med Assoc J. 2023; 195: E1040. |
| [20] | Yang S, Liu D, Song H. Ivermectin: An effective treatment for cutaneous larva migrans. Trop Med Infect Dis. 2022; 7(3): 15-21. |
| [21] | Kumar A, Sharma P, Garg S. Treatment outcomes in cutaneous larva migrans: Albendazole vs. Ivermectin. J Dermatol. 2023; 47(2): 210-216. |
| [22] | Nagaraja K, et al. The use of thiabendazole in treating cutaneous larva migrans. J Indian Med Assoc. 2018; 116(4): 239-242. |
| [23] | Ferreira F, et al. Adverse effects of thiabendazole in the treatment of cutaneous larva migrans. J Trop Med. 2021; 42(3): 174-177. |
| [24] | Corbett E, et al. Cryotherapy in the treatment of cutaneous larva migrans: a review of 50 cases. J Dermatol Surg. 2019; 45(6): 897-902. |
| [25] | Loze M, et al. The efficacy of antihistamines in treating cutaneous larva migrans. Clin Infect Dis. 2020; 28(8): 1014-1020. |
| [26] | Singer E, et al. Corticosteroids in the management of cutaneous larva migrans. J Dermatol Therapy. 2021; 43(9): 1124-1129. |
| [27] | Decker B, et al. Management of secondary bacterial infections in cutaneous larva migrans patients. Ann Clin Infect Dis. 2021; 56(4): 142-148. |
| [28] | Schär F, Trostdorf U, Giardina F, Khieu V, Muth S, Marti H, et al. Strongyloides stercoralis: Global distribution and risk factors. PLoS Negl Trop Dis. 2013; 7(7): e2288. |
APA Style
Broshtilova, V., Yungareva, I., Velevska-Vatova, Y., Trenovski, A., Marina, S. (2025). Cutaneous Larva Migrans - Clinical Case and Literature Review. International Journal of Clinical Dermatology, 8(1), 33-39. https://doi.org/10.11648/j.ijcd.20250801.16
ACS Style
Broshtilova, V.; Yungareva, I.; Velevska-Vatova, Y.; Trenovski, A.; Marina, S. Cutaneous Larva Migrans - Clinical Case and Literature Review. Int. J. Clin. Dermatol. 2025, 8(1), 33-39. doi: 10.11648/j.ijcd.20250801.16
@article{10.11648/j.ijcd.20250801.16,
author = {Valentina Broshtilova and Irina Yungareva and Yoanna Velevska-Vatova and Aleksandar Trenovski and Sonya Marina},
title = {Cutaneous Larva Migrans - Clinical Case and Literature Review
},
journal = {International Journal of Clinical Dermatology},
volume = {8},
number = {1},
pages = {33-39},
doi = {10.11648/j.ijcd.20250801.16},
url = {https://doi.org/10.11648/j.ijcd.20250801.16},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcd.20250801.16},
abstract = {Cutaneous larva migrans is a parasitic disease typical of tropical and subtropical climate zones. In Bulgaria, cases are rare and are usually found in tourists who have visited the tropics. The disease is caused by nematode larvae, most often Ancylostoma braziliense. Humans are accidental hosts in which the larvae do not reach sexual maturity, do not complete their life cycle and die. Infection occurs through contact with contaminated soil or sand or by ingestion of nematode eggs. There are two types of larva migrans: cutaneous and visceral. The cutaneous form manifests itself with characteristic itchy, erythematous, linear or zigzag crawling lesions, while the visceral form affects internal organs such as the liver, lungs, heart and brain and is more common in children without hygiene habits. The diagnosis of the cutaneous form is based on exposure history and clinical presentation, while the visceral form requires serological tests and imaging studies. We present a 61-year-old female patient with cutaneous larva migrans acquired after travel to Zanzibar. The diagnosis was based on the typical clinical presentation, epidemiological history, and histopathological findings. Laboratory tests revealed moderate blood eosinophilia and elevated inflammatory markers. Systemic treatment with ivermectin led to rapid symptom relief and complete recovery. This case highlights the importance of early diagnosis and treatment in patients returning from endemic areas.
},
year = {2025}
}
TY - JOUR T1 - Cutaneous Larva Migrans - Clinical Case and Literature Review AU - Valentina Broshtilova AU - Irina Yungareva AU - Yoanna Velevska-Vatova AU - Aleksandar Trenovski AU - Sonya Marina Y1 - 2025/06/19 PY - 2025 N1 - https://doi.org/10.11648/j.ijcd.20250801.16 DO - 10.11648/j.ijcd.20250801.16 T2 - International Journal of Clinical Dermatology JF - International Journal of Clinical Dermatology JO - International Journal of Clinical Dermatology SP - 33 EP - 39 PB - Science Publishing Group SN - 2995-1305 UR - https://doi.org/10.11648/j.ijcd.20250801.16 AB - Cutaneous larva migrans is a parasitic disease typical of tropical and subtropical climate zones. In Bulgaria, cases are rare and are usually found in tourists who have visited the tropics. The disease is caused by nematode larvae, most often Ancylostoma braziliense. Humans are accidental hosts in which the larvae do not reach sexual maturity, do not complete their life cycle and die. Infection occurs through contact with contaminated soil or sand or by ingestion of nematode eggs. There are two types of larva migrans: cutaneous and visceral. The cutaneous form manifests itself with characteristic itchy, erythematous, linear or zigzag crawling lesions, while the visceral form affects internal organs such as the liver, lungs, heart and brain and is more common in children without hygiene habits. The diagnosis of the cutaneous form is based on exposure history and clinical presentation, while the visceral form requires serological tests and imaging studies. We present a 61-year-old female patient with cutaneous larva migrans acquired after travel to Zanzibar. The diagnosis was based on the typical clinical presentation, epidemiological history, and histopathological findings. Laboratory tests revealed moderate blood eosinophilia and elevated inflammatory markers. Systemic treatment with ivermectin led to rapid symptom relief and complete recovery. This case highlights the importance of early diagnosis and treatment in patients returning from endemic areas. VL - 8 IS - 1 ER -
Department of Internal Medicine, Pharmacology and Clinical Pharmacology, Pediatrics, Epidemiology, Infectious and Skin Diseases, Faculty of Medicine, Sofia University “St. Kliment Ohridski”, Sofia, Bulgaria
Department of Dermatology and Venereology Diseases, Medical Institute of the Ministry of Internal Affairs, Sofia, Bulgaria
Department of Infectious Diseases, Parasitology and Dermatovenereology, Medical University, Varna, Bulgaria
Department of Anesthesiology and Intensive Care, Medical Institute of the Ministry of Internal Affairs, Sofia, Bulgaria
Diagnostic and Consultative Sector, Medical Institute of the Ministry of Internal Affairs, Sofia, Bulgaria
Information