Introduction: QuadMix is considered to be one of the most powerful class of anti-erectile dysfunction agents and superior to all forms of intracavernosal injections especially in men with permanent/severe erectile dysfunction (ED) that has defiled oral therapy. QuadMix consists of papaverine HCl, phentolamine mesylate, prostaglandin E1 and atropine sulfate designed to act synergistically with satisfactory endpoint. We report our preliminary experience with QuadMIX in the management of permanent/severe ED. Methodology: This is a prospective study which was carried out between July 2020 to June 2022. Two questionnaires (a proforma and IIEF-5) were administered to all patients presenting with ED to objectively assess the etiology, risk factors and severity of ED without bias. Only patients who met the inclusion criteria were recruited for the study and informed consent was obtained. Individual test dose was calculated and the patients were subsequently trained on self-injection using an autoinjector. Two capsules of phenylephrine were also given to the patients to keep with them with appropriate instructions. Data obtained were analyzed using Statistical Package for Social Sciences version 20.0. P value of less than 0.005 was considered statistically significant. Results: Sixty patients were enrolled for the study. All patient had either permanent ED or severe ED. Thirty percent had radical prostatectomy surgery. Ten percent had trauma with pelvic bone involvement while 31.66%, 3.34% and 25% had comorbid conditions (diabetes mellitus and hypertension), prolonged priapism and no obvious organic etiology respectively. Forty percent of the patients failed to achieve satisfactory erection on oral medication while 60% had no erection despite taking phosphodiesterase type 5 inhibitors (PDE5i). All patients had tumescence for satisfactory sexual intercourse within 10 mins following administration of QuadMix. Fifty eight patients (96.67%) had spontaneous detumescence after ejaculation. Only 2 patients (3.34%) had priapism. One was reversed with ejaculation, use of ice pack around the perineum and caps phenylephrine while the second patient had intracavernosal aspiration to achieve detumescence. Conclusion: QuadMix is an effective and safe agent in the treatment of permanent and severe ED in patients with comorbid condition. It also improves quality of life (QoL) and sexual performance in patient who has had permanent ED following radical prostatectomy.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Erectile dysfunction (ED) is defined as persistent inability to achieve and maintain an erection sufficient for satisfactory intercourse
[1]
Kenenna Obiatuegwu, Terkaa Atim, Sadiq Abu et al. Correlation between the Severity of Erectile Dysfunction and Prostate Size in Patients with Benign Prostatic Enlargement. Afr J Urol 27, 31 (2021),
. he prevalence and severity of ED increases as men grow older from 9% in men younger than 40 years to 71% in men older than 70 years
[2]
Morant S, Bloomfield G, Vat V et al. Increased Sexual Dysfunction in Men with Storage and Voiding Lower Urinary Tract Symptoms. J Sex. Med. 2009; 6 (4): 1103-1110.
.The incidence per age distribution is 31% for patients aged 50-59 years and as high as 76% for patients aged 70-80 years
[3]
Raymond C, Francois G and Culley C. Sexual Dysfunction and Lower Urinary Tract Symptoms Associated Benign Prostatic Hyperplasia. European Urol. 2005; 47 (6): 824-837.
.ED affects sexual performance and can lead to significant marital disharmony among couples with negative impact on QoL
[1]
Kenenna Obiatuegwu, Terkaa Atim, Sadiq Abu et al. Correlation between the Severity of Erectile Dysfunction and Prostate Size in Patients with Benign Prostatic Enlargement. Afr J Urol 27, 31 (2021),
The etiology of ED can be categorized as organic, psychogenic and mixed ED endorsed by the International Society of Impotence Research
[4]
Anthony J. Bella, Tom F. Lue. Male Sexual Dysfunction. In: Smith’s General Urology. Emil A. T, Jack W. M. Ch.38, 17th edition: McGraw Hill (Lange), 2008; 589-610.
[4]
. Organic ED consists of neurogenic, hormonal, arterial, cavernosal (venogenic) and drug related including antiandrogens used in the treatment of benign prostatic enlargement. Neurogenic ED results from peripheral (cavernous and pudendal nerve) or central pathologies (spinal cord injury, dementia, stroke, brain tumors and Shy-Drager syndrome). Iatrogenic trauma from radical prostatectomy and abdominal perineal resection can result in ED from direct injury to cavernous or pudendal nerves
[1]
Kenenna Obiatuegwu, Terkaa Atim, Sadiq Abu et al. Correlation between the Severity of Erectile Dysfunction and Prostate Size in Patients with Benign Prostatic Enlargement. Afr J Urol 27, 31 (2021),
Anthony J. Bella, Tom F. Lue. Male Sexual Dysfunction. In: Smith’s General Urology. Emil A. T, Jack W. M. Ch.38, 17th edition: McGraw Hill (Lange), 2008; 589-610.
[1, 4]
.This results to permanent ED with patients requiring major interventions like intracavernosal injection or penile surgery.
Hormonal disorder including hypogonadism due to hypothalamic or pituitary tumor, estrogen or androgen therapy or orchidectomy can suppress sexual drive and nocturnal erection. Veronelli et al noted that hyperprolactinemia, Cushing’s syndrome, hyperthyroidism, hypothyroidism and Addison’s disease can suppress libido and result in severe forms of ED due to hormonal fluctuations
[5]
Veronelli, A., Masu, A., Ranieri, R. et al. Prevalence of Erectile Dysfunction in Thyroid Disorders: Comparison with Control Subjects and with Obese and Diabetic Patients. Int J Impot Res 18, 111–114 (2006).
. Arteriogenic injury to the tunica albuginea following neglected penile fracture can affect the arterial supply to the penis including the hypogastric, cavernous or helicine arteries with consequent decrease flow to sinusoidal spaces thus decreasing rigidity or prolonging time to maximal erection resulting in severe ED in most cases
[1]
Kenenna Obiatuegwu, Terkaa Atim, Sadiq Abu et al. Correlation between the Severity of Erectile Dysfunction and Prostate Size in Patients with Benign Prostatic Enlargement. Afr J Urol 27, 31 (2021),
.Certain drugs including centrally acting antihypertensives, antiandrogens and antidepressants can affect the serotonergic, noradrenagic and dopaminergic pathways of erection
[1]
Kenenna Obiatuegwu, Terkaa Atim, Sadiq Abu et al. Correlation between the Severity of Erectile Dysfunction and Prostate Size in Patients with Benign Prostatic Enlargement. Afr J Urol 27, 31 (2021),
. Antiandrogens modulates sexual desire via central nervous system androgen receptors with consequent ED.Performance anxiety, strained relationship and depression can either cause or aggravate ED. Possible mechanism may be due to an imbalance of central neurotransmitters or over inhibition of spinal erection center in the brain
[4]
Anthony J. Bella, Tom F. Lue. Male Sexual Dysfunction. In: Smith’s General Urology. Emil A. T, Jack W. M. Ch.38, 17th edition: McGraw Hill (Lange), 2008; 589-610.
[4]
. However mixed ED remains the most common type of ED and it is a combination of both organic and psychogenic ED
[1]
Kenenna Obiatuegwu, Terkaa Atim, Sadiq Abu et al. Correlation between the Severity of Erectile Dysfunction and Prostate Size in Patients with Benign Prostatic Enlargement. Afr J Urol 27, 31 (2021),
Anthony J. Bella, Tom F. Lue. Male Sexual Dysfunction. In: Smith’s General Urology. Emil A. T, Jack W. M. Ch.38, 17th edition: McGraw Hill (Lange), 2008; 589-610.
[1, 4]
.
A commonly used validated questionnaire for assessing the severity of ED is the 15-item International Index of Erectile Function (IIEF). This has been simplified to a 5-item version (IIEF-5) which is more suited for casual or office purpose. Sexual function assessed with IIEF-5 includes erectile function, orgasmic function, sexual desire, intercourse satisfaction and overall satisfaction. ED severity is classified as severe (5-7), moderate (8-11), mild to moderate (12-16), mild (17-21), and no ED (22-25)
[7]
Rosen R. C. Evaluation of the Patient with Erectile Dysfunction: History, Questionnaires and Physical Examination. Endocrine 2004; 23(2-3): 107-111.
.Severe or permanent ED is likely to defile oral medication compared to intracavernosal agents.
ED affects the QoL of significant number of aging male population, hence addressing the risk factors through lifestyle modification as well as medical and surgical interventions will reduce the physical and psychological impact of ED with satisfactory QoL and sexual performance
[8]
Pastuszak AW. Current Diagnosis and Management of Erectile Dysfunction. Curr Sex Health Rep. 2014 Sep; 6(3): 164-176.
The management ED can be challenging and entails a detail medical and sexual history, clinical examination and targeted investigations including fasting blood sugar, fasting lipid profile, hormonal profile, penile color splash and prostate-specific antigen (PSA) test especially in men above the age of 50. The treatment of ED ranges from lifestyle modification, treatment of comorbid conditions and organic dysfunction, psychosexual therapy as well as the use of certain drugs and intracavernosal agents such as alprostadil, Bimix, Trimix and more recent powerful Quadmix. The use of penile vacuum device is not generally accepted due to convenience couple with the fact that it works for only selected group of patients
[17]
Opsomer RJ, Wese FX, De Groote P, Van Cangh PJ. The external vacuum device in the management of erectile dysfunction. Acta Urol Belg. 1997 Dec; 65(4): 13-6.
[17]
. Over 60% of men with ED including those with hypertension, diabetes, and spinal cord trauma can achieve satisfactory erection for penetrative sexual intercourse with phosphodiesterase type 5 inhibitors (PDE5i) including sildenafil, tadalafil, vardenafil and avanafil
[9]
McMahon CG. Current Diagnosis and Management of Erectile Dysfunction. Med J Aust. 2019 Jun; 210(10): 469-476.
. Intraurethral agents and self-administered intracavernosal injection therapy using vasodilator drugs such as alprostadil is an effective treatment with less systemic side effect compared to oral medications. These agents are useful in men who fail to respond to oral medications and in most cases preferred in tropical Africa compared to surgery
[9]
McMahon CG. Current Diagnosis and Management of Erectile Dysfunction. Med J Aust. 2019 Jun; 210(10): 469-476.
. Surgical treatment of ED with either malleable of a more physiological multicomponent inflatable penile implants is associated with high satisfaction rates but not without its untoward effect, availability of device and license for use in tropical Africa as well as high cost of device and expertise. Penile arterial revascularization and venous ligation surgery are associated with poor outcome. Shock wave therapy seems to be effective in men with penile atherosclerotic disease but availability remains an issue in tropical Africa,
QuadMix is a patient-administered intracavernosal injection currently considered as one of the most powerful class of agents in the treatment of erectile dysfunction (ED). Quad-Mix contains four drugs designed to act synergistically
[11]
Chung E. A Review of Current and Emerging Therapeutic Options for Erectile Dysfunction. Med Sci (Basel). 2019 Aug 29; 7(9): 91.
. This includes Papaverine, Phentolamine, Alprostadil, and Atropine. Papaverine is a potent vasodilator. It causes blood vessels to expand and produces erection by causing increase in blood flow to the penis. Phentolamine relaxes and dilates blood vessels with increased cardiac ouput. This can induce an erection when injected into the corpora body of the penis. Prostaglandin E1 such as Alprostadil is also a potent agent that induces erection by relaxing blood vessels in the penis while dilating the cavernosal arteries which will lead to increased arterial inflow velocity with increased venous resistance
[11]
Chung E. A Review of Current and Emerging Therapeutic Options for Erectile Dysfunction. Med Sci (Basel). 2019 Aug 29; 7(9): 91.
. The end result will lead to increased blood accumulation with more blood flowing into the penis compared to the rate of outflow. Atropine Sulfate inhibits the receptors in the nervous system that control smooth muscle relaxation which invariably increases arterial blood flow to the penis.
Future research into the molecular mechanisms of ED and development of improved medications with minimal systemic side effects will be exciting to our growing number of men with ED. This will invariably expand the significant armamentarium of treatments currently available, thus invariably improve the QoL and sexual performance of affected men and by extension their partners.
2. Methodology
This is a prospective randomized study which was commenced in July 2020 and ended in June 2022. All patients presenting to urology clinic with erectile dysfunction were counseled on the study and proforma/IIEF-5 issued to objectively assess the severity of ED. Informed consent was obtained from those that met the inclusion criteria.
2.1. Inclusion Criteria
1. All consenting patients.
2. Patient with severe ED.
3. Patient with permanent ED after surgery including radical prostatectomy
2.2. Exclusion Criteria
1. Patients with mild to moderate, mild ED or no ED.
2. Patients with significant urinary incontinence following radical prostatectomy.
3. Patient on urethral catheter.
Two questionnaires (a proforma and standard abridged version of International Index of Erectile Function -IIEF-5) were administered to all consenting patients to objectively assess the etiology, risk factors and severity of ED without bias. Individual test dose for each patient were determined by the authors in clinic and the patients were subsequently trained on self-injection using an autoinjector as shown in Figure 1 below.
The agent was issued as per dose in a sterile autoinjector fitted syringe. Two capsules of phenylephrine were also given to the patients to keep with them with appropriate instructions. Patients were counseled to take the phenylephrine capsules if erection persists after 2 hours and to contact the urology team involved in the study via phone. Data obtained were analyzed using Statistical Package for Social Sciences version 20.0. P value of less than 0.05 was be considered statistically significant.
Figure 1. Autoinjector to ease self-administration.
3. Results
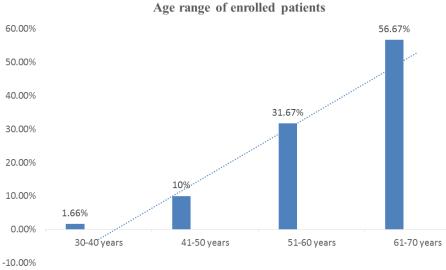
Sixty patients were enrolled for the study. The enrolled patients fell within the age ranges of 37 to 69 years with a mean age of 58.04 ± 7.25. One patient (1.66%) fell within the age ranges of 30-40 years while six patients (10%) were between the age ranges of 41-50 years. Those that fell within the age range of 51-60, and 61-70 years were 31.67% and 56.67% respectively as shown in Figure 2 below.
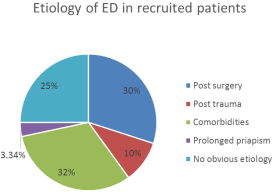
All patient enrolled for the study had either permanent ED or severe ED. Severe ED refers to those that have IIEF-5 score of 5-7 while permanent ED refers to a subset of severe ED patients with IIEF-5 score of 5 alone and have never experienced any form of erection with no libido. Eighteen patients (30%) had radical prostatectomy surgery for localized prostate cancer. Six patients (10%) had trauma with pelvic bone involvement while 19 (31.66%), 2 (3.34%) and 15(25%) patients had comorbid conditions (diabetes mellitus and hypertension), prolonged priapism and no obvious organic etiology respectively as shown in Figure 2.
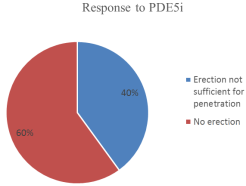
Forty percent of the patients failed to achieve satisfactory erection on oral medication while 60% had no erection despite taking phosphodiesterase type 5 inhibitors (PDE5i) as shown in Figure 4.
Figure 4. Response to ingestion of phosphodiesterase type 5 inhibitors (PDE5i).
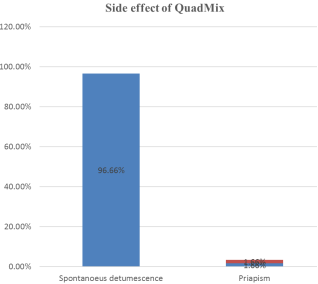
All patients had tumescence for satisfactory sexual intercourse with QuadMix within 10 mins following administration of QuadMix into the coporal body. Fifty eight patients (96.67%) had spontaneous detumescence after ejaculation. Only 2 patients (3.34%) had priapism as shown in Figure 5.
One was reversed with ejaculation, use of ice pack around the perineum and caps phenylephrine while the second patient had intracavernosal aspiration to achieve detumescence as depicted in Figure 5.
4. Discussion
QuadMix is a patient-administered intracavernosal injection currently considered as one of the most powerful class of agents in the treatment of erectile dysfunction (ED) that defiled oral medications. Quad-Mix contains four drugs designed to act synergistically
[10]
Super Quad-Mix 5 ml vial (lyophilized) | Defy Medical
. This includes Papaverine, Phentolamine, Alprostadil, and Atropine. Anthony J. Bella et al reported that more than half of men aged 40–70 years in the United States find it difficult to attain or maintain penile erection necessary for satisfactory penetrative sexual performance
[4]
Anthony J. Bella, Tom F. Lue. Male Sexual Dysfunction. In: Smith’s General Urology. Emil A. T, Jack W. M. Ch.38, 17th edition: McGraw Hill (Lange), 2008; 589-610.
[4]
This shows that ED is common and requires special attention especially because of the negative impact on quality of life (QoL) with respect to sexual adventure and performance. Our study confirmed that Quadmix is a potent viable agent with no systemic side effect and was effective in all patient with permanent or severe ED that defiled oral therapy.
We found that our patients fell within the age ranges of 37-69 years. This further confirms the age range reported by Anthony J Bella et al
[4]
Anthony J. Bella, Tom F. Lue. Male Sexual Dysfunction. In: Smith’s General Urology. Emil A. T, Jack W. M. Ch.38, 17th edition: McGraw Hill (Lange), 2008; 589-610.
[4]
. Our study noted that the incidence of ED increased with age as only one patient (1.66%) fell within the age ranges of 30-40 years while it increased exponentially with 10%, 31.67% and 56.67% falling within the age ranges of 41-50, 51-60, and 61-70 years respectively. This is in keeping with finding by Obiatuegwu K et al which reported that incidence of erectile dysfunction increases with age and incidence skyrocketed in recent times
[1]
Kenenna Obiatuegwu, Terkaa Atim, Sadiq Abu et al. Correlation between the Severity of Erectile Dysfunction and Prostate Size in Patients with Benign Prostatic Enlargement. Afr J Urol 27, 31 (2021),
McMahon et al reported the epidemiological data from Australian, American and Britain and established that ED manifests more with aging. Their observational study puts the prevalence of ED as 5% amongst men below 40 years and 30–40% amongst men above 60 years
[9]
McMahon CG. Current Diagnosis and Management of Erectile Dysfunction. Med J Aust. 2019 Jun; 210(10): 469-476.
.Though we focused more on patients with severe or permanent ED we observed the same exponential trend as the age of our patient increases.
The factors responsible for ED in this study varied from radical prostatectomy, hypertension/diabetes mellitus, perineal trauma and prolonged priapism. These caused permanent/ severe ED that seriously interfered with the QoL and sexual performance of all the patients. We must also state that the patients who had ED secondary to radical prostatectomy anticipated same and was counseled before surgery. Despite their awareness on inevitable ED as a complication post radical prostatectomy they were excited that QuadMix was a viable solution to their sexual dysfunction with no systemic untoward effect. Many studies reported similar etiologies with our study
[1]
Kenenna Obiatuegwu, Terkaa Atim, Sadiq Abu et al. Correlation between the Severity of Erectile Dysfunction and Prostate Size in Patients with Benign Prostatic Enlargement. Afr J Urol 27, 31 (2021),
Morant S, Bloomfield G, Vat V et al. Increased Sexual Dysfunction in Men with Storage and Voiding Lower Urinary Tract Symptoms. J Sex. Med. 2009; 6 (4): 1103-1110.
Raymond C, Francois G and Culley C. Sexual Dysfunction and Lower Urinary Tract Symptoms Associated Benign Prostatic Hyperplasia. European Urol. 2005; 47 (6): 824-837.
Erectile dysfunction is also associated with LUTS due to benign prostatic enlargement (BPE)
[1]
Kenenna Obiatuegwu, Terkaa Atim, Sadiq Abu et al. Correlation between the Severity of Erectile Dysfunction and Prostate Size in Patients with Benign Prostatic Enlargement. Afr J Urol 27, 31 (2021),
Morant S, Bloomfield G, Vat V et al. Increased Sexual Dysfunction in Men with Storage and Voiding Lower Urinary Tract Symptoms. J Sex. Med. 2009; 6 (4): 1103-1110.
Raymond C, Francois G and Culley C. Sexual Dysfunction and Lower Urinary Tract Symptoms Associated Benign Prostatic Hyperplasia. European Urol. 2005; 47 (6): 824-837.
. The severity of LUTS due to BPE can be assessed with IPPS. Majority of our patients were above 50 years and BPE is common after the age of 50 as well. Obiatuegwu et al reported that ED due to BPE was not permanent/severe and can be comfortable addressed with daily low dose tadanafil. Quadmix was not used in this category of patients as we focused more on patients with permanent/severe ED. Moon et al also noted a positive relationship between ED and comorbidities including obesity
[16]
Moon KH, Park SY, Kim YW. Obesity and Erectile Dysfunction: From Bench to Clinical Implication. World J Mens Health. 2019 May; 37(2): 138-147.
.Though we did not focus on BMI but we noted that significant number of our patients had hypertension/diabetes.
Several options of management for erectile dysfunction are available ranging from the first line use of the phosphodiesterase type 5 inhibitors (PDE5i), use of intracavernosal agents, vacuum constrictive device as well as surgical options including implants and revascularization surgeries/interventions
[8]
Pastuszak AW. Current Diagnosis and Management of Erectile Dysfunction. Curr Sex Health Rep. 2014 Sep; 6(3): 164-176.
Peter GC, Mathias H, Patricia G, Joseph N, John PM. A review of outcomes of an intacavernosal injection therapy programme. BJU int. 2012; 110(11): 1787-1791.
[15]
Duncan C, Omran GJ, Teh J, Davis NF, Bolton DM, Lawrentschuk N. Erectile dysfunction: a global review of intracavernosal injectables. World J Urol. 2019 Jun; 37(6): 1007-1014.
.In the past, most patient are started on step ladder therapy with oral phosphodiesterase type 5 inhibitors and then progressively step up to more invasive procedures. Currently such protocol is discouraged and patients addressed on their merit considering their peculiar etiology/risk factor of ED. Pastuszak et al reported that oral PDE5i achieves a good responses for men with arteriogenic ED with overall satisfactory of 78.1%. Our patients did not achieve tumescence on PGE5i and we were more concerned on the systemic side effect of PDE5i compared to QuadMix that demonstrated safe systemic profile. We do not agree with Pastuszak et al and will only recommend oral PDE5i for younger men with ED as older men are likely to be on certain medications for comorbid conditions that may invariably lead to drug interaction with untoward effect. All our patients never complained of any systemic issues and were very satisfied with the outcome of QuadMix with respect to QoL and performance. More so, if all patients achieved tumescence in clinic even without high libido, we envisage a stronger erection when they are alone and probably in the mood for sexual intercourse. This further shows that QuadMix remains a potent and viable agent with no systemic side effect.
A multicenter study which assessed the outcome and complications of Bimix in 157 men reported a response rate of 94% with a side effect incidence of 0.9–2.6 % for prolonged erection, pain, or hematoma
[8]
Pastuszak AW. Current Diagnosis and Management of Erectile Dysfunction. Curr Sex Health Rep. 2014 Sep; 6(3): 164-176.
. In our experience, all patients had tumescence for satisfactory sexual intercourse with QuadMix within 10 mins following administration of into the corporal body. Over Ninety six percent (96.67%) had spontaneous detumescence after ejaculation and only 3.34% had mild priapism. This is in keeping with by Pastuszak et al who reported similar satisfactory response to intracavernosal injection. We did not observe any other side effects like haematoma, fibrosis and scarring in our study this may be due to the difference in agents used as QuadMix contains extra two agents designed to counter the adverse effects of each other.
Clinical guidelines supports the use of combination intracavernosal therapy as an alternative to a single agent due to its more favorable side-effect profile with attendant higher efficacy and sexual performance
[11]
Chung E. A Review of Current and Emerging Therapeutic Options for Erectile Dysfunction. Med Sci (Basel). 2019 Aug 29; 7(9): 91.
Al-Adl, A. M., Abdel-Wahab, O., El-Karamany, T., & Aal, A. A. (2011). Combined intracavernous vasoactive drugs and sildenafil citrate in treatment of severe erectile dysfunction not responding to on-demand monotherapy. Arab Journal of Urology, 9(2), 153–158.
. This is unlike the other intracavernosal injections which are mainly indicated for arteriogenic erectile dysfunction
[12]
Ashraf HF, Yasser E, Hosam H, Shady Z, Rany S. A study of the possible effects of repeated intracorporeal self-injection of vasoactive drugs in patients with elevated end diastolic velocity during pharmacopenile duplex ultrasonography. Cent European J Urol. 2013; 66(2): 210-214.
[13]
Al-Adl, A. M., Abdel-Wahab, O., El-Karamany, T., & Aal, A. A. (2011). Combined intracavernous vasoactive drugs and sildenafil citrate in treatment of severe erectile dysfunction not responding to on-demand monotherapy. Arab Journal of Urology, 9(2), 153–158.
. Though we did not set out to assess the effect of Quadmix on repeated injections, we found QuadMix highly effective for both arteriogenic and venoocclusve erectile dysfunction.
We also noted that QuadMix was also effective for nerve injury after radical prostatectomy as well as patients with hypertension/diabetes. The QoL of all our patients post radical prostatectomy as per sexual performance as well as relationship with their partners improved. This further confirms that QuadMix remains a potent and most powerful intracavernosal agent with no systemic side effect and satisfactory endpoint in all our patients.
5. Conclusion
Sexuality is a vital aspect of relationship and ED can pose a negative impact on QoL and sexual performance. QuadMix is an effective and safe agent in the treatment of permanent and severe erectile dysfunction with comorbid condition. It also improves quality of life (QoL) and sexual performance in patient who has had radical prostatectomy. The ease of administration, the efficacy and good safety profile makes it one of the choicest treatment option for erectile dysfunction.
Abu Sadiq: Conceptualization, Funding acquisition, Validation, Visualization
Funding
This article was funded by the authors.
Conflict of Interest
The authors declare no conflicts of interest.
References
[1]
Kenenna Obiatuegwu, Terkaa Atim, Sadiq Abu et al. Correlation between the Severity of Erectile Dysfunction and Prostate Size in Patients with Benign Prostatic Enlargement. Afr J Urol 27, 31 (2021),
Morant S, Bloomfield G, Vat V et al. Increased Sexual Dysfunction in Men with Storage and Voiding Lower Urinary Tract Symptoms. J Sex. Med. 2009; 6 (4): 1103-1110.
Raymond C, Francois G and Culley C. Sexual Dysfunction and Lower Urinary Tract Symptoms Associated Benign Prostatic Hyperplasia. European Urol. 2005; 47 (6): 824-837.
Anthony J. Bella, Tom F. Lue. Male Sexual Dysfunction. In: Smith’s General Urology. Emil A. T, Jack W. M. Ch.38, 17th edition: McGraw Hill (Lange), 2008; 589-610.
[5]
Veronelli, A., Masu, A., Ranieri, R. et al. Prevalence of Erectile Dysfunction in Thyroid Disorders: Comparison with Control Subjects and with Obese and Diabetic Patients. Int J Impot Res 18, 111–114 (2006).
Ashraf HF, Yasser E, Hosam H, Shady Z, Rany S. A study of the possible effects of repeated intracorporeal self-injection of vasoactive drugs in patients with elevated end diastolic velocity during pharmacopenile duplex ultrasonography. Cent European J Urol. 2013; 66(2): 210-214.
[13]
Al-Adl, A. M., Abdel-Wahab, O., El-Karamany, T., & Aal, A. A. (2011). Combined intracavernous vasoactive drugs and sildenafil citrate in treatment of severe erectile dysfunction not responding to on-demand monotherapy. Arab Journal of Urology, 9(2), 153–158.
Peter GC, Mathias H, Patricia G, Joseph N, John PM. A review of outcomes of an intacavernosal injection therapy programme. BJU int. 2012; 110(11): 1787-1791.
[15]
Duncan C, Omran GJ, Teh J, Davis NF, Bolton DM, Lawrentschuk N. Erectile dysfunction: a global review of intracavernosal injectables. World J Urol. 2019 Jun; 37(6): 1007-1014.
Opsomer RJ, Wese FX, De Groote P, Van Cangh PJ. The external vacuum device in the management of erectile dysfunction. Acta Urol Belg. 1997 Dec; 65(4): 13-6.
Kenenna, O., Terkaa, A., Felix, M., Christopher, O., Okwudili, A., et al. (2025). OuadMix Penile Injection: An Initial Urologists Experience. International Journal of Clinical Urology, 9(1), 73-79. https://doi.org/10.11648/j.ijcu.20250901.22
Kenenna O, Terkaa A, Felix M, Christopher O, Okwudili A, et al. OuadMix Penile Injection: An Initial Urologists Experience. Int J Clin Urol. 2025;9(1):73-79. doi: 10.11648/j.ijcu.20250901.22
@article{10.11648/j.ijcu.20250901.22,
author = {Obiatuegwu Kenenna and Atim Terkaa and Magnus Felix and Otabor Christopher and Amu Okwudili and Abu Sadiq},
title = {OuadMix Penile Injection: An Initial Urologists Experience
},
journal = {International Journal of Clinical Urology},
volume = {9},
number = {1},
pages = {73-79},
doi = {10.11648/j.ijcu.20250901.22},
url = {https://doi.org/10.11648/j.ijcu.20250901.22},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcu.20250901.22},
abstract = {Introduction: QuadMix is considered to be one of the most powerful class of anti-erectile dysfunction agents and superior to all forms of intracavernosal injections especially in men with permanent/severe erectile dysfunction (ED) that has defiled oral therapy. QuadMix consists of papaverine HCl, phentolamine mesylate, prostaglandin E1 and atropine sulfate designed to act synergistically with satisfactory endpoint. We report our preliminary experience with QuadMIX in the management of permanent/severe ED. Methodology: This is a prospective study which was carried out between July 2020 to June 2022. Two questionnaires (a proforma and IIEF-5) were administered to all patients presenting with ED to objectively assess the etiology, risk factors and severity of ED without bias. Only patients who met the inclusion criteria were recruited for the study and informed consent was obtained. Individual test dose was calculated and the patients were subsequently trained on self-injection using an autoinjector. Two capsules of phenylephrine were also given to the patients to keep with them with appropriate instructions. Data obtained were analyzed using Statistical Package for Social Sciences version 20.0. P value of less than 0.005 was considered statistically significant. Results: Sixty patients were enrolled for the study. All patient had either permanent ED or severe ED. Thirty percent had radical prostatectomy surgery. Ten percent had trauma with pelvic bone involvement while 31.66%, 3.34% and 25% had comorbid conditions (diabetes mellitus and hypertension), prolonged priapism and no obvious organic etiology respectively. Forty percent of the patients failed to achieve satisfactory erection on oral medication while 60% had no erection despite taking phosphodiesterase type 5 inhibitors (PDE5i). All patients had tumescence for satisfactory sexual intercourse within 10 mins following administration of QuadMix. Fifty eight patients (96.67%) had spontaneous detumescence after ejaculation. Only 2 patients (3.34%) had priapism. One was reversed with ejaculation, use of ice pack around the perineum and caps phenylephrine while the second patient had intracavernosal aspiration to achieve detumescence. Conclusion: QuadMix is an effective and safe agent in the treatment of permanent and severe ED in patients with comorbid condition. It also improves quality of life (QoL) and sexual performance in patient who has had permanent ED following radical prostatectomy.
},
year = {2025}
}
TY - JOUR
T1 - OuadMix Penile Injection: An Initial Urologists Experience
AU - Obiatuegwu Kenenna
AU - Atim Terkaa
AU - Magnus Felix
AU - Otabor Christopher
AU - Amu Okwudili
AU - Abu Sadiq
Y1 - 2025/04/29
PY - 2025
N1 - https://doi.org/10.11648/j.ijcu.20250901.22
DO - 10.11648/j.ijcu.20250901.22
T2 - International Journal of Clinical Urology
JF - International Journal of Clinical Urology
JO - International Journal of Clinical Urology
SP - 73
EP - 79
PB - Science Publishing Group
SN - 2640-1355
UR - https://doi.org/10.11648/j.ijcu.20250901.22
AB - Introduction: QuadMix is considered to be one of the most powerful class of anti-erectile dysfunction agents and superior to all forms of intracavernosal injections especially in men with permanent/severe erectile dysfunction (ED) that has defiled oral therapy. QuadMix consists of papaverine HCl, phentolamine mesylate, prostaglandin E1 and atropine sulfate designed to act synergistically with satisfactory endpoint. We report our preliminary experience with QuadMIX in the management of permanent/severe ED. Methodology: This is a prospective study which was carried out between July 2020 to June 2022. Two questionnaires (a proforma and IIEF-5) were administered to all patients presenting with ED to objectively assess the etiology, risk factors and severity of ED without bias. Only patients who met the inclusion criteria were recruited for the study and informed consent was obtained. Individual test dose was calculated and the patients were subsequently trained on self-injection using an autoinjector. Two capsules of phenylephrine were also given to the patients to keep with them with appropriate instructions. Data obtained were analyzed using Statistical Package for Social Sciences version 20.0. P value of less than 0.005 was considered statistically significant. Results: Sixty patients were enrolled for the study. All patient had either permanent ED or severe ED. Thirty percent had radical prostatectomy surgery. Ten percent had trauma with pelvic bone involvement while 31.66%, 3.34% and 25% had comorbid conditions (diabetes mellitus and hypertension), prolonged priapism and no obvious organic etiology respectively. Forty percent of the patients failed to achieve satisfactory erection on oral medication while 60% had no erection despite taking phosphodiesterase type 5 inhibitors (PDE5i). All patients had tumescence for satisfactory sexual intercourse within 10 mins following administration of QuadMix. Fifty eight patients (96.67%) had spontaneous detumescence after ejaculation. Only 2 patients (3.34%) had priapism. One was reversed with ejaculation, use of ice pack around the perineum and caps phenylephrine while the second patient had intracavernosal aspiration to achieve detumescence. Conclusion: QuadMix is an effective and safe agent in the treatment of permanent and severe ED in patients with comorbid condition. It also improves quality of life (QoL) and sexual performance in patient who has had permanent ED following radical prostatectomy.
VL - 9
IS - 1
ER -
Kenenna, O., Terkaa, A., Felix, M., Christopher, O., Okwudili, A., et al. (2025). OuadMix Penile Injection: An Initial Urologists Experience. International Journal of Clinical Urology, 9(1), 73-79. https://doi.org/10.11648/j.ijcu.20250901.22
Kenenna O, Terkaa A, Felix M, Christopher O, Okwudili A, et al. OuadMix Penile Injection: An Initial Urologists Experience. Int J Clin Urol. 2025;9(1):73-79. doi: 10.11648/j.ijcu.20250901.22
@article{10.11648/j.ijcu.20250901.22,
author = {Obiatuegwu Kenenna and Atim Terkaa and Magnus Felix and Otabor Christopher and Amu Okwudili and Abu Sadiq},
title = {OuadMix Penile Injection: An Initial Urologists Experience
},
journal = {International Journal of Clinical Urology},
volume = {9},
number = {1},
pages = {73-79},
doi = {10.11648/j.ijcu.20250901.22},
url = {https://doi.org/10.11648/j.ijcu.20250901.22},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcu.20250901.22},
abstract = {Introduction: QuadMix is considered to be one of the most powerful class of anti-erectile dysfunction agents and superior to all forms of intracavernosal injections especially in men with permanent/severe erectile dysfunction (ED) that has defiled oral therapy. QuadMix consists of papaverine HCl, phentolamine mesylate, prostaglandin E1 and atropine sulfate designed to act synergistically with satisfactory endpoint. We report our preliminary experience with QuadMIX in the management of permanent/severe ED. Methodology: This is a prospective study which was carried out between July 2020 to June 2022. Two questionnaires (a proforma and IIEF-5) were administered to all patients presenting with ED to objectively assess the etiology, risk factors and severity of ED without bias. Only patients who met the inclusion criteria were recruited for the study and informed consent was obtained. Individual test dose was calculated and the patients were subsequently trained on self-injection using an autoinjector. Two capsules of phenylephrine were also given to the patients to keep with them with appropriate instructions. Data obtained were analyzed using Statistical Package for Social Sciences version 20.0. P value of less than 0.005 was considered statistically significant. Results: Sixty patients were enrolled for the study. All patient had either permanent ED or severe ED. Thirty percent had radical prostatectomy surgery. Ten percent had trauma with pelvic bone involvement while 31.66%, 3.34% and 25% had comorbid conditions (diabetes mellitus and hypertension), prolonged priapism and no obvious organic etiology respectively. Forty percent of the patients failed to achieve satisfactory erection on oral medication while 60% had no erection despite taking phosphodiesterase type 5 inhibitors (PDE5i). All patients had tumescence for satisfactory sexual intercourse within 10 mins following administration of QuadMix. Fifty eight patients (96.67%) had spontaneous detumescence after ejaculation. Only 2 patients (3.34%) had priapism. One was reversed with ejaculation, use of ice pack around the perineum and caps phenylephrine while the second patient had intracavernosal aspiration to achieve detumescence. Conclusion: QuadMix is an effective and safe agent in the treatment of permanent and severe ED in patients with comorbid condition. It also improves quality of life (QoL) and sexual performance in patient who has had permanent ED following radical prostatectomy.
},
year = {2025}
}
TY - JOUR
T1 - OuadMix Penile Injection: An Initial Urologists Experience
AU - Obiatuegwu Kenenna
AU - Atim Terkaa
AU - Magnus Felix
AU - Otabor Christopher
AU - Amu Okwudili
AU - Abu Sadiq
Y1 - 2025/04/29
PY - 2025
N1 - https://doi.org/10.11648/j.ijcu.20250901.22
DO - 10.11648/j.ijcu.20250901.22
T2 - International Journal of Clinical Urology
JF - International Journal of Clinical Urology
JO - International Journal of Clinical Urology
SP - 73
EP - 79
PB - Science Publishing Group
SN - 2640-1355
UR - https://doi.org/10.11648/j.ijcu.20250901.22
AB - Introduction: QuadMix is considered to be one of the most powerful class of anti-erectile dysfunction agents and superior to all forms of intracavernosal injections especially in men with permanent/severe erectile dysfunction (ED) that has defiled oral therapy. QuadMix consists of papaverine HCl, phentolamine mesylate, prostaglandin E1 and atropine sulfate designed to act synergistically with satisfactory endpoint. We report our preliminary experience with QuadMIX in the management of permanent/severe ED. Methodology: This is a prospective study which was carried out between July 2020 to June 2022. Two questionnaires (a proforma and IIEF-5) were administered to all patients presenting with ED to objectively assess the etiology, risk factors and severity of ED without bias. Only patients who met the inclusion criteria were recruited for the study and informed consent was obtained. Individual test dose was calculated and the patients were subsequently trained on self-injection using an autoinjector. Two capsules of phenylephrine were also given to the patients to keep with them with appropriate instructions. Data obtained were analyzed using Statistical Package for Social Sciences version 20.0. P value of less than 0.005 was considered statistically significant. Results: Sixty patients were enrolled for the study. All patient had either permanent ED or severe ED. Thirty percent had radical prostatectomy surgery. Ten percent had trauma with pelvic bone involvement while 31.66%, 3.34% and 25% had comorbid conditions (diabetes mellitus and hypertension), prolonged priapism and no obvious organic etiology respectively. Forty percent of the patients failed to achieve satisfactory erection on oral medication while 60% had no erection despite taking phosphodiesterase type 5 inhibitors (PDE5i). All patients had tumescence for satisfactory sexual intercourse within 10 mins following administration of QuadMix. Fifty eight patients (96.67%) had spontaneous detumescence after ejaculation. Only 2 patients (3.34%) had priapism. One was reversed with ejaculation, use of ice pack around the perineum and caps phenylephrine while the second patient had intracavernosal aspiration to achieve detumescence. Conclusion: QuadMix is an effective and safe agent in the treatment of permanent and severe ED in patients with comorbid condition. It also improves quality of life (QoL) and sexual performance in patient who has had permanent ED following radical prostatectomy.
VL - 9
IS - 1
ER -