Introduction: Premature ejaculation is one of the major disorders of sexual functions in males. The prevalence rate of 25-40% has been reported across all age groups globally. Ejaculation latency is affected by psychosomatic factors which may include obesity but the relationship between PE and obesity have not been well documented in sub-Saharan Africa. This study evaluates the prevalence of PE and correlation between PE and body mass index. Methods: This is a prospective cross-sectional study carried out in Federal Capital Territory (FCT) Abuja, Nigeria over a period of 2 years from January 2019 to December 2020. By simple random sampling, participants were recruited for the study. Two questionnaires (a proforma and PEDT) were administered to all the participants who gave consent to be enrolled and met the inclusion criteria. Two basic anthropometric measurements (weight and height) were objectively obtained. Data obtained were analyzed using Statistical Package for Social Sciences version 20.0. P value of less than 0.05 was considered statistically significant. Results: A total of 426 persons participated in the study. Majority of the participants (51.88%) fell within the age range of 20-30 years, while seventy-five participants (17.61%) were between the age ranges of 31-40 years. Those that fell within the age range of 41-50, 51-60, and 61-70 years were 16.43%, 8.22% and 5.87% respectively. Seventy-two participants (16.9%) had PE while three hundred and six participants (71.83%) had no PE. Probable/borderline PE was noted in 48 (11.27%) participants. Mean age of participants with PE was 27.88 years while the mean age of participants with borderline PE was 25.67 years. Mean age of participants with no PE was 41.85 years. Sixty-seven participants (15.73%) were obese, 131 (30.75%) were overweight while 228 (53.52%) had normal BMI. Amongst the participants who had PE, 48 (66.67%) had normal BMI, 16 (22.22%) were overweight while 8 (11.11%) were obese. Majority of participants (66.67%) with probable/borderline PE had normal BMI, 16.67% were overweight while 16.67% were obese. P value of less than 0.05 was significant. Conclusion: This study shows that premature ejaculation is common amongst all age group and has a variable relationship with body habitus, possibly dependent on the sub-type of premature ejaculation. There was an inverse correlation between PE and BMI in younger populations which suggests a lifelong sub-type. PE was also commoner in leaner younger participants and the number of participants with PE decreased as BMI increased.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Premature Ejaculation, Sexual Dysfunction, Body Mass Index, Obesity
1. Introduction
Premature ejaculation (PE) is one of the major disorders of sexual functions in males. PE is defined as loss or absence of ejaculatory control, marked distress or interpersonal difficulty and by a short intra-vaginal ejaculatory latency time (IELT)
[1]
Stanley Althof. The Psychology of Premature Ejaculation: Therapies and Consequences. J Sex Med. 2006 Sep: 3 Suppl 4: 324-31.
. The prevalence rate of 25-40% has been reported across all age groups globally
[2]
Porst H, Montorsi F, Rosen R. C., Gaynor L, Grupe S, Alexander J. The Premature Ejaculation Prevalence and Attitudes (PEPA) Survey: Prevalence, Comorbidities, and Professional Help-Seeking. Eur. Urol. 2007; 51: 816–824.
. Premature ejaculation is a social issue that has negative impact on the quality of life (QoL) and sexual performance
[3]
Eric Chung, Brent Gilbert, Marlon Perera, Matthew J Roberts. Premature Ejaculation: A Clinical Review for the General Physician. Aust Fam Physician, 2015 Oct; 44(10): 737-743.
[3]
. PE may potentially impact negatively on sexual life leading to psychological distress, low self- esteem, anxiety disorder, mild to severe erectile dysfunction and low libido
[3]
Eric Chung, Brent Gilbert, Marlon Perera, Matthew J Roberts. Premature Ejaculation: A Clinical Review for the General Physician. Aust Fam Physician, 2015 Oct; 44(10): 737-743.
[3]
. Many patients seems reluctant to volunteer information regarding their sexual dysfunction including PE despite the psychological and social impact on QoL and performance with negative impact in interpersonal relationships with their partners. This aspect of male sexual dysfunction is under reported or ignored because most patients with PE either feel embarrassed and most time they present to the wrong clinician or seek other nonorthodox or alternative means.
There is no clear consensus on the definition of PE and many authors feel it should be tailored to individuals
[4]
Nicholas Gillman, Michael Gillman. Premature Ejaculation: Aetiology and Treatment Strategies. Med Sci (Basel). 2019 Oct 25; 7(11): 102.
. In 2007, the International Society for Sexual Medicine (ISSM) formed an adhoc committee saddled with the role of providing evidence-based and unified definition of PE. This committee came together and established three key criteria including intra-vaginal ejaculation latency time (IELT), lack of ejaculatory control and negative personal consequences
[4]
Nicholas Gillman, Michael Gillman. Premature Ejaculation: Aetiology and Treatment Strategies. Med Sci (Basel). 2019 Oct 25; 7(11): 102.
. In 2013 a consensus was reached by the Committee to define PE as a male sexual dysfunction characterized by:
1) Ejaculation which always or nearly always occurs prior to or within about one minute of vaginal penetration from the first sexual experience (lifelong), or, a clinically significant reduction in latency time, often to about 3 min or less (acquired).
2) The inability to delay ejaculation on all or nearly all vaginal penetrations.
3) Negative personal consequences, such as distress, bother, frustration and/or the avoidance of sexual intimacy
[5]
Serefoglu E. C., McMahon C. G., Waldinger M. D., Althof S. E., Shindel A., Adaikan G., Becher E. F., Dean J., Giuliano F., Hellstrom W. J. G., et al. An Evidence-Based Unified Definition of Lifelong and Acquired Premature Ejaculation: Report of the Second International Society for Sexual Medicine Ad Hoc Committee for the Definition of Premature Ejaculation. J. Sex. Med. 2014; 11: 1423–1441.
Lifelong PE is characterized by low IELT, usually less than one minute, from the first sexual experience, and on most, if not all, subsequent encounters which suggests in most cases a functional disturbance, familial origin with possible genetic polymorphisms
[1]
Stanley Althof. The Psychology of Premature Ejaculation: Therapies and Consequences. J Sex Med. 2006 Sep: 3 Suppl 4: 324-31.
Janssen P. K., Schaik R. V., Olivier B., Waldinger M. D. The 5-HT2C receptor gene Cys23Ser polymorphism influences the intravaginal ejaculation latency time in Dutch Caucasian men with lifelong premature ejaculation. Asian J. Androl. 2014; 16: 607–610.
.Acquired PE refers to reduced ejaculatory latency that develops at some point in life in patients who had normal ejaculations in the past. This may be due to an identifiable medical, psychological or interpersonal, psycho-relational, endocrine and urologic dysfunction including prostatitis and hyperthyroidism
[7]
McMahon C. G., Jannini E. A., Serefoglu E. C., Hellstrom W. J. G. The pathophysiology of acquired premature ejaculation. Transl. Androl. Urol. 2016; 5: 434–449.
Waldinger and Schweitzer recognized the need for tailored definition and further classified PE into as lifelong (primary), acquired (secondary), variable and subjective
[8]
Waldinger M. D., Schweitzer D. H. The Use of Old and Recent DSM Definitions of Premature Ejaculation in Observational Studies: A Contribution to the Present Debate for a New Classification of PE in the DSM-V. J. Sex. Med. 2005; 5: 1079–1087.
.They noted that the true prevalence of PE was much less than previously reported prevalence rates. Based on these, two separate observational and cross-sectional studies involving two countries arrived at an overall prevalence of 19.8% and 25.80%
[9]
Serefoglu EC, Yaman O, Cayan S, et al. Prevalence of the complaint of ejaculating prematurely and the four premature ejaculation syndromes: results from the Turkish Society of Andrology Sexual Health Survey. J Sex Med 2011; 8: 540-8.
Gao J, Zhang X, Su P, et al. Prevalence and factors associated with the complaint of premature ejaculation and the four premature ejaculation syndromes: a large observational study in China. J Sex Med 2013; 10: 1874-81.
. The prevalence rates of specific and tailored PE was found to be 2.3% and 3.2% for lifelong PE, 3.9% and 4.5% for acquired PE, 8.5% and 11.4% for variable PE and 5.1% and 6.4% for subjective PE
[9]
Serefoglu EC, Yaman O, Cayan S, et al. Prevalence of the complaint of ejaculating prematurely and the four premature ejaculation syndromes: results from the Turkish Society of Andrology Sexual Health Survey. J Sex Med 2011; 8: 540-8.
Gao J, Zhang X, Su P, et al. Prevalence and factors associated with the complaint of premature ejaculation and the four premature ejaculation syndromes: a large observational study in China. J Sex Med 2013; 10: 1874-81.
. Treatment seeking pattern as well as traditional beliefs especially in tropical Africa may contribute to variations in reported rates of PE, as it is possible that men with lifelong PE could resolve to live with the problem and not seek intervention compared to men with acquired PE who are likely to be have more psychological burden and will consequently seek redress.
Ejaculation latency is affected by psychosomatic factors which may include obesity but the relationship between PE and obesity has not been well documented in sub-Saharan Africa. Prevalence of obesity is increasing in sub-sahara Africa and characterized by increased mass of adipose tissue. Obesity is also associated with certain syndromes including impaired glucose tolerance (IGT) or type 2 diabetes mellitus (DM), hypertension and other heart diseases. Leptin which is protein majorly secreted by the adipose tissue that was discovered by Freidman's group who reported the cloning of the obese gene responsible for the typical phenotype of obesity. Apart from metabolic and neuroendocrine hormone functions, Leptin also has a role in body weight regulation. Body mass index (BMI) and fat mass has a direct relationship with plasma Leptin level in humans which is synthesized by fat cells
[12]
Maffei M, Halaas J, Ravussin E, Pratley RE, Lee GH et al. Leptin levels in human and rodent: measurement of plasma leptin and ob RNA in obese and weight reduced subjects. Nature Medicine 1995; 1: 1155- 1161.
[12]
.
Ahmet Gokce et al reported a lower prevalence of PE in subjects that are overweight or obese, but the difference was only significant according to obesity (19.5% vs 2.1%, p<0.01) probably due to the small sample size of the study
[13]
Ahmet Gokce, Mehmet Rami Helvaci, Orhan Veli Ozkan, Hasan Kaya. Obesity and Primary Premature Ejaculation. January 2008. 17: 159-162.
This study evaluates the prevalence of PE and correlation between PE and body mass index.
2. Methodology
This is a prospective cross-sectional study carried out in Federal Capital Territory (FCT) Abuja, Nigeria over a period of 2 years from January 2019 to December 2020. By simple random sampling, participants were recruited for the study. During these period all consenting subjects who met the inclusion criteria were recruited for the study.
2.1. Inclusion Criteria
1) All consenting subjects.
2) Subjects above the age of 20.
2.2. Exclusion Criteria
1) Subject who did not give consent.
2) Subjects with erectile dysfunction (ED).
3) Subjects with co-morbid conditions like hypertension and diabetes mellitus.
4) Subjects on urethral catheter.
A structured questionnaire (Premature Ejaculation Diagnostic Tool -PEDT) was utilized. A proforma was also designed to obtain the relevant information, viz. biodata, and age, comorbid conditions including hypertension, diabetes mellitus, coronary heart disease, myocardial infarction and obesity. The weight and height of consenting subjects were objectively obtained with a mobile weighing scale and stadiometer respectively. The 2 questionnaires (proforma and PEDT) were administered to those that met the inclusion criteria. Those who could not read English language were assigned an interpreter.
Completed questionnaire/proforma of all eligible subjects were collated and the data analyzed using Statistical Package for the Social Sciences (SPSS) version 20.0 and P values less than 0.05 were considered to be statistically significant. Student’s paired T test and Chi-square were used to compare means where appropriate. The relationship between PE and body mass index was determined using the Pearson’s correlation. The result is represented in the form of tables and charts.
3. Results
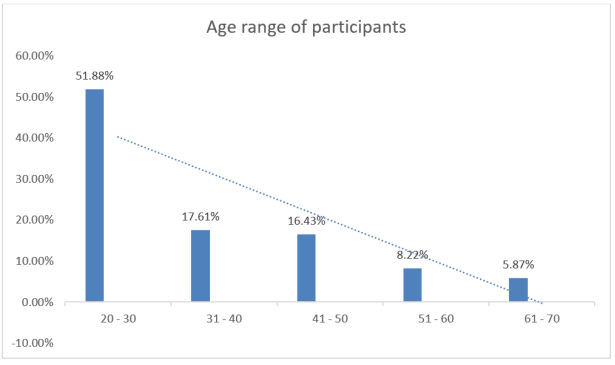
Four hundred and twenty six patients who met the inclusion criteria were enrolled and participated in the study. The participants fell within the age ranges of 23 to 67years. Majority of the participants (51.88%) fell within the age ranges of 20-30 years while seventy-five participants (17.61%) were between the age ranges of 31-40years. Those that fell within the age range of 41-50, 51-60, and 61-70 years were 16.43%, 8.22% and 5.87% respectively. Majority of the participants were young and perhaps more sexually active compared to older participants as shown in Figure 1.
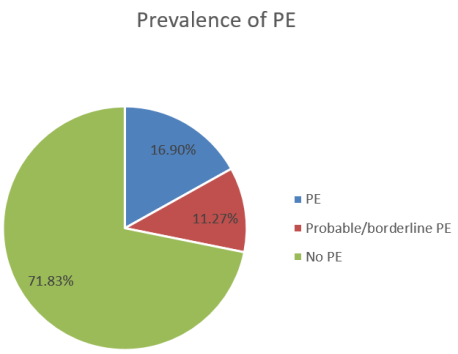
Seventy-two participants (16.9%) had PE, probable/borderline PE was noted in 48 (11.27%) participants, while 306 participants (71.83%) had no PE and felt they were normal as show figure 2.
Figure 2. Prevalence of premature ejaculation among the participants.
Mean age of participants with PE was 27.88 ± 7.07 while the mean age of participants with borderline PE was 25.67 ± 7.26. Mean age of participants with no PE was 41.85 ± 5.16 as shown in Table 1.
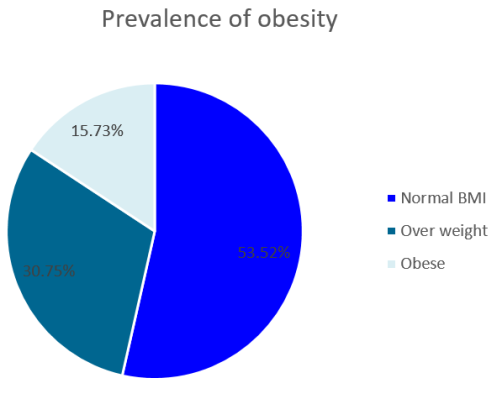
Figure 3. Prevalence of obesity amongst participants.
Sixty-seven participants (15.73%) were obese, 131 (30.75%) were overweight while 228 (53.52%) had normal BMI as shown in figure 3.
Amongst the participants who had PE, 48 (66.67%) had normal BMI, 16 (22.22%) were overweight while 8 (11.11%) were obese as shown in Table 2 below.
Table 2. Correlation between BMI and PE.
BMI
Frequency (n=72)
Prevalence of PE (%)
Normal BMI
48
66.67
Over weight
16
22.22
Obese
8
11.11
P value = 0.211.
Majority of participants (66.67%) with probable/borderline PE had normal BMI, 16.67% were overweight while 16.67% were obese as shown in table 3 below. P value of less than 0.05 was significant.
Table 3. Correlation between BMI and borderline PE.
BMI
Frequency (n=48)
Prevalence of borderline PE (%)
Normal BMI
32
66.67
Over weight
8
16.67
Obese
8
16.67
P value = 0.224.
Table 4. Summary of relationship between BMI and PE.
Pearson’s r-value
p-value
Interpretation
BMI versus PE
-0.269
0.113
Weak negative correlation
4. Discussion
Premature ejaculation (PE) is one of the major disorders of sexual functions in males. PE is defined as loss or absence of ejaculatory control, marked distress or interpersonal difficulty and by a short intra-vaginal ejaculatory latency time (IELT)
[1]
Stanley Althof. The Psychology of Premature Ejaculation: Therapies and Consequences. J Sex Med. 2006 Sep: 3 Suppl 4: 324-31.
. Premature ejaculation is a male sexual dysfunction and can affect the QoL and sexual performance of individual and by extension their partners. The true prevalence of premature ejaculation is difficult to ascertain especially in tropical Africa where the locals are not willing to discuss their sexual dysfunction due to potential stigmatization. Generally acquired premature ejaculation is commoner in the older age group who have likelihood of comorbidities
[7]
McMahon C. G., Jannini E. A., Serefoglu E. C., Hellstrom W. J. G. The pathophysiology of acquired premature ejaculation. Transl. Androl. Urol. 2016; 5: 434–449.
while the lifelong PE tends to be common amongst the younger population
[14]
David LR, Zsuzsanna K, Krisztina H. Age-related differences in the prevalence of premature ejaculation; taking a second and more detailed look. Sexual medicine. 2024; 12(4): 057.
[14]
. Our study only analyzed the generally prevalence of PE irrespective of the subtypes as we focused only on the prevalence of PE in the general population.
Porst H et al reported a prevalence rate of 25-40% across all age groups globally
[2]
Porst H, Montorsi F, Rosen R. C., Gaynor L, Grupe S, Alexander J. The Premature Ejaculation Prevalence and Attitudes (PEPA) Survey: Prevalence, Comorbidities, and Professional Help-Seeking. Eur. Urol. 2007; 51: 816–824.
. The prevalence of PE in our study was 16.9% and those with probable/borderline PE had a prevalence of 11.27% thus putting the overall prevalence to be at 28.17%. This is within the globally reported prevalence rate of 25-40%,
[2]
Porst H, Montorsi F, Rosen R. C., Gaynor L, Grupe S, Alexander J. The Premature Ejaculation Prevalence and Attitudes (PEPA) Survey: Prevalence, Comorbidities, and Professional Help-Seeking. Eur. Urol. 2007; 51: 816–824.
most likely due to the fact that majority of our study populations were young subjects and invariably sexually active. McMahon C. G et al reported similar prevalence rate is amongst younger populations with lifelong PE
[7]
McMahon C. G., Jannini E. A., Serefoglu E. C., Hellstrom W. J. G. The pathophysiology of acquired premature ejaculation. Transl. Androl. Urol. 2016; 5: 434–449.
Furthermore the prevalence of PE can vary depending on the actual definition adopted in arriving at the diagnosis. In 2013 a consensus was reached by the Committee to define PE as a male sexual dysfunction characterized by ejaculation which always or nearly always occurs prior to or within about one minute of vaginal penetration from the first sexual experience (lifelong), or, a clinically significant reduction in latency time, often to about 3 min or less (acquired) or the inability to delay ejaculation on all or nearly all vaginal penetrations
[5]
Serefoglu E. C., McMahon C. G., Waldinger M. D., Althof S. E., Shindel A., Adaikan G., Becher E. F., Dean J., Giuliano F., Hellstrom W. J. G., et al. An Evidence-Based Unified Definition of Lifelong and Acquired Premature Ejaculation: Report of the Second International Society for Sexual Medicine Ad Hoc Committee for the Definition of Premature Ejaculation. J. Sex. Med. 2014; 11: 1423–1441.
.The prevalence tends to be higher in prospective cross sectional studies carried out using the PEDT questionnaire compared to prospective studies where the actual timing for making the diagnosis was controlled and unified according to the definition by ISSM
[14]
David LR, Zsuzsanna K, Krisztina H. Age-related differences in the prevalence of premature ejaculation; taking a second and more detailed look. Sexual medicine. 2024; 12(4): 057.
[14]
.Our index study was a cross sectional study utilizing the PEDT questionnaires, hence patients subjectivity could be contributory to the observed high prevalence rate.
Furthermore in our study, we found that PE was more common in leaner participants and the number of participants with PE decreased as BMI increased and obese patients in our study had lower prevalence compared to participants with normal BMI. This may be explained by the observation that the majority of our study participants were younger persons with age range of 20-30 years and perhaps not likely to have added much weight at that age. Younger subjects are less likely to have comorbidities like overweight, obesity, diabetes mellitus and other endocrine disorders compared to older subjects. More so, since our study did not focus on the prevalence of the subtypes of PE we cannot make similar assertion on prevalence with respect to the subtypes as it varies with age.
Some studies corroborate our findings
[15]
Enis RC, Burak O. Premature ejaculation and endocrine disorders. A literature review. World J Mens Health. 2021; 40(1): 38-51.
[16]
Gokce A, Ekmekcioglu O. Insight on pathogenesis of lifelong premature ejaculation: Inverse relationship between lifelong premature ejaculation and obesity. Int J impot Res. 2010; 22(4): 251-254.
[17]
Yavuz G. Comparison of acquired and lifelong premature ejaculation and predictive values of acquired premature ejaculation in clinical presentation: A clinical study. Ann med Res. 2021; 28(5): 897-902.
[15-17]
. Enis RC et al reported that higher values of serum testosterone were found in younger patients with lifelong premature ejaculation in contrast to lower levels of serum testosterone seen in older men with acquired premature ejaculation and concurrent comorbidity with increased BMI
[15]
Enis RC, Burak O. Premature ejaculation and endocrine disorders. A literature review. World J Mens Health. 2021; 40(1): 38-51.
[15]
. Our study also reported higher prevalence in younger participants most probably due to hormonal level of testosterone in keeping with the findings by Enis RC et al.
Gokce A et al in another study involving younger population on the relationship between obesity and PE found that the prevalence of life long premature ejaculation increased as the BMI decreases in the participants
[16]
Gokce A, Ekmekcioglu O. Insight on pathogenesis of lifelong premature ejaculation: Inverse relationship between lifelong premature ejaculation and obesity. Int J impot Res. 2010; 22(4): 251-254.
[16]
. This is in keeping with our finding which showed that PE was more common in leaner participants compared to those that are either overweight or obese. Some other studies have shown that with increasing BMI the prevalence of premature ejaculation increased
[9]
Serefoglu EC, Yaman O, Cayan S, et al. Prevalence of the complaint of ejaculating prematurely and the four premature ejaculation syndromes: results from the Turkish Society of Andrology Sexual Health Survey. J Sex Med 2011; 8: 540-8.
Gao J, Zhang X, Su P, et al. Prevalence and factors associated with the complaint of premature ejaculation and the four premature ejaculation syndromes: a large observational study in China. J Sex Med 2013; 10: 1874-81.
Serefoglu EC, Yaman O, Cayan S, et al. The comparison of premature ejaculation assessment questionnaires and their sensitivity for the four premature ejaculation syndromes: results from the Turkish society of andrology sexual health survey. J Sex Med 2011; 8: 1177-85.
. This invariably shows that the relationship between BMI and premature ejaculation may depend on the subtype of premature ejaculation being discussed whether lifelong or acquired premature ejaculation. However a closer look at these studies suggest that the sub-type of premature ejaculation being described is the acquired sub-type as the patients were older with concurrent comorbidity like diabetes mellitus, metabolic syndromes and obesity.
It is believed that increasing BMI with the attendant generous amount of adipose tissues in the body comes with other disorders like insulin resistance, leading to type 2 diabetes mellitus. Also levels of testosterone tends to be low as well as increase in other endocrine disorders. This invariably increases the risk of erectile dysfunction as well as acquired premature ejaculation
[9]
Serefoglu EC, Yaman O, Cayan S, et al. Prevalence of the complaint of ejaculating prematurely and the four premature ejaculation syndromes: results from the Turkish Society of Andrology Sexual Health Survey. J Sex Med 2011; 8: 540-8.
Gao J, Zhang X, Su P, et al. Prevalence and factors associated with the complaint of premature ejaculation and the four premature ejaculation syndromes: a large observational study in China. J Sex Med 2013; 10: 1874-81.
Serefoglu EC, Yaman O, Cayan S, et al. The comparison of premature ejaculation assessment questionnaires and their sensitivity for the four premature ejaculation syndromes: results from the Turkish society of andrology sexual health survey. J Sex Med 2011; 8: 1177-85.
This study shows that premature ejaculation is common amongst all age group and has a variable relationship with body habitus possibly dependent on the subtype of premature ejaculation. There was an inverse correlation between PE and BMI in younger populations with possibly a lifelong subtype of PE. PE was also more common in leaner younger participants and the number of participants with PE decreased as BMI increased.
Porst H, Montorsi F, Rosen R. C., Gaynor L, Grupe S, Alexander J. The Premature Ejaculation Prevalence and Attitudes (PEPA) Survey: Prevalence, Comorbidities, and Professional Help-Seeking. Eur. Urol. 2007; 51: 816–824.
Eric Chung, Brent Gilbert, Marlon Perera, Matthew J Roberts. Premature Ejaculation: A Clinical Review for the General Physician. Aust Fam Physician, 2015 Oct; 44(10): 737-743.
[4]
Nicholas Gillman, Michael Gillman. Premature Ejaculation: Aetiology and Treatment Strategies. Med Sci (Basel). 2019 Oct 25; 7(11): 102.
Serefoglu E. C., McMahon C. G., Waldinger M. D., Althof S. E., Shindel A., Adaikan G., Becher E. F., Dean J., Giuliano F., Hellstrom W. J. G., et al. An Evidence-Based Unified Definition of Lifelong and Acquired Premature Ejaculation: Report of the Second International Society for Sexual Medicine Ad Hoc Committee for the Definition of Premature Ejaculation. J. Sex. Med. 2014; 11: 1423–1441.
Janssen P. K., Schaik R. V., Olivier B., Waldinger M. D. The 5-HT2C receptor gene Cys23Ser polymorphism influences the intravaginal ejaculation latency time in Dutch Caucasian men with lifelong premature ejaculation. Asian J. Androl. 2014; 16: 607–610.
McMahon C. G., Jannini E. A., Serefoglu E. C., Hellstrom W. J. G. The pathophysiology of acquired premature ejaculation. Transl. Androl. Urol. 2016; 5: 434–449.
Waldinger M. D., Schweitzer D. H. The Use of Old and Recent DSM Definitions of Premature Ejaculation in Observational Studies: A Contribution to the Present Debate for a New Classification of PE in the DSM-V. J. Sex. Med. 2005; 5: 1079–1087.
Serefoglu EC, Yaman O, Cayan S, et al. Prevalence of the complaint of ejaculating prematurely and the four premature ejaculation syndromes: results from the Turkish Society of Andrology Sexual Health Survey. J Sex Med 2011; 8: 540-8.
Gao J, Zhang X, Su P, et al. Prevalence and factors associated with the complaint of premature ejaculation and the four premature ejaculation syndromes: a large observational study in China. J Sex Med 2013; 10: 1874-81.
Serefoglu EC, Yaman O, Cayan S, et al. The comparison of premature ejaculation assessment questionnaires and their sensitivity for the four premature ejaculation syndromes: results from the Turkish society of andrology sexual health survey. J Sex Med 2011; 8: 1177-85.
Maffei M, Halaas J, Ravussin E, Pratley RE, Lee GH et al. Leptin levels in human and rodent: measurement of plasma leptin and ob RNA in obese and weight reduced subjects. Nature Medicine 1995; 1: 1155- 1161.
[13]
Ahmet Gokce, Mehmet Rami Helvaci, Orhan Veli Ozkan, Hasan Kaya. Obesity and Primary Premature Ejaculation. January 2008. 17: 159-162.
David LR, Zsuzsanna K, Krisztina H. Age-related differences in the prevalence of premature ejaculation; taking a second and more detailed look. Sexual medicine. 2024; 12(4): 057.
[15]
Enis RC, Burak O. Premature ejaculation and endocrine disorders. A literature review. World J Mens Health. 2021; 40(1): 38-51.
[16]
Gokce A, Ekmekcioglu O. Insight on pathogenesis of lifelong premature ejaculation: Inverse relationship between lifelong premature ejaculation and obesity. Int J impot Res. 2010; 22(4): 251-254.
[17]
Yavuz G. Comparison of acquired and lifelong premature ejaculation and predictive values of acquired premature ejaculation in clinical presentation: A clinical study. Ann med Res. 2021; 28(5): 897-902.
Kenenna, O., Terkaa, A., Felix, M., Christopher, O., Sadiq, A. (2025). Premature Ejaculation: Prevalence and Relationship with Body Mass Index. International Journal of Clinical Urology, 9(1), 101-106. https://doi.org/10.11648/j.ijcu.20250901.27
Kenenna, O.; Terkaa, A.; Felix, M.; Christopher, O.; Sadiq, A. Premature Ejaculation: Prevalence and Relationship with Body Mass Index. Int. J. Clin. Urol.2025, 9(1), 101-106. doi: 10.11648/j.ijcu.20250901.27
Kenenna O, Terkaa A, Felix M, Christopher O, Sadiq A. Premature Ejaculation: Prevalence and Relationship with Body Mass Index. Int J Clin Urol. 2025;9(1):101-106. doi: 10.11648/j.ijcu.20250901.27
@article{10.11648/j.ijcu.20250901.27,
author = {Obiatuegwu Kenenna and Atim Terkaa and Magnus Felix and Otabor Christopher and Abu Sadiq},
title = {Premature Ejaculation: Prevalence and Relationship with Body Mass Index
},
journal = {International Journal of Clinical Urology},
volume = {9},
number = {1},
pages = {101-106},
doi = {10.11648/j.ijcu.20250901.27},
url = {https://doi.org/10.11648/j.ijcu.20250901.27},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcu.20250901.27},
abstract = {Introduction: Premature ejaculation is one of the major disorders of sexual functions in males. The prevalence rate of 25-40% has been reported across all age groups globally. Ejaculation latency is affected by psychosomatic factors which may include obesity but the relationship between PE and obesity have not been well documented in sub-Saharan Africa. This study evaluates the prevalence of PE and correlation between PE and body mass index. Methods: This is a prospective cross-sectional study carried out in Federal Capital Territory (FCT) Abuja, Nigeria over a period of 2 years from January 2019 to December 2020. By simple random sampling, participants were recruited for the study. Two questionnaires (a proforma and PEDT) were administered to all the participants who gave consent to be enrolled and met the inclusion criteria. Two basic anthropometric measurements (weight and height) were objectively obtained. Data obtained were analyzed using Statistical Package for Social Sciences version 20.0. P value of less than 0.05 was considered statistically significant. Results: A total of 426 persons participated in the study. Majority of the participants (51.88%) fell within the age range of 20-30 years, while seventy-five participants (17.61%) were between the age ranges of 31-40 years. Those that fell within the age range of 41-50, 51-60, and 61-70 years were 16.43%, 8.22% and 5.87% respectively. Seventy-two participants (16.9%) had PE while three hundred and six participants (71.83%) had no PE. Probable/borderline PE was noted in 48 (11.27%) participants. Mean age of participants with PE was 27.88 years while the mean age of participants with borderline PE was 25.67 years. Mean age of participants with no PE was 41.85 years. Sixty-seven participants (15.73%) were obese, 131 (30.75%) were overweight while 228 (53.52%) had normal BMI. Amongst the participants who had PE, 48 (66.67%) had normal BMI, 16 (22.22%) were overweight while 8 (11.11%) were obese. Majority of participants (66.67%) with probable/borderline PE had normal BMI, 16.67% were overweight while 16.67% were obese. P value of less than 0.05 was significant. Conclusion: This study shows that premature ejaculation is common amongst all age group and has a variable relationship with body habitus, possibly dependent on the sub-type of premature ejaculation. There was an inverse correlation between PE and BMI in younger populations which suggests a lifelong sub-type. PE was also commoner in leaner younger participants and the number of participants with PE decreased as BMI increased.
},
year = {2025}
}
TY - JOUR
T1 - Premature Ejaculation: Prevalence and Relationship with Body Mass Index
AU - Obiatuegwu Kenenna
AU - Atim Terkaa
AU - Magnus Felix
AU - Otabor Christopher
AU - Abu Sadiq
Y1 - 2025/06/20
PY - 2025
N1 - https://doi.org/10.11648/j.ijcu.20250901.27
DO - 10.11648/j.ijcu.20250901.27
T2 - International Journal of Clinical Urology
JF - International Journal of Clinical Urology
JO - International Journal of Clinical Urology
SP - 101
EP - 106
PB - Science Publishing Group
SN - 2640-1355
UR - https://doi.org/10.11648/j.ijcu.20250901.27
AB - Introduction: Premature ejaculation is one of the major disorders of sexual functions in males. The prevalence rate of 25-40% has been reported across all age groups globally. Ejaculation latency is affected by psychosomatic factors which may include obesity but the relationship between PE and obesity have not been well documented in sub-Saharan Africa. This study evaluates the prevalence of PE and correlation between PE and body mass index. Methods: This is a prospective cross-sectional study carried out in Federal Capital Territory (FCT) Abuja, Nigeria over a period of 2 years from January 2019 to December 2020. By simple random sampling, participants were recruited for the study. Two questionnaires (a proforma and PEDT) were administered to all the participants who gave consent to be enrolled and met the inclusion criteria. Two basic anthropometric measurements (weight and height) were objectively obtained. Data obtained were analyzed using Statistical Package for Social Sciences version 20.0. P value of less than 0.05 was considered statistically significant. Results: A total of 426 persons participated in the study. Majority of the participants (51.88%) fell within the age range of 20-30 years, while seventy-five participants (17.61%) were between the age ranges of 31-40 years. Those that fell within the age range of 41-50, 51-60, and 61-70 years were 16.43%, 8.22% and 5.87% respectively. Seventy-two participants (16.9%) had PE while three hundred and six participants (71.83%) had no PE. Probable/borderline PE was noted in 48 (11.27%) participants. Mean age of participants with PE was 27.88 years while the mean age of participants with borderline PE was 25.67 years. Mean age of participants with no PE was 41.85 years. Sixty-seven participants (15.73%) were obese, 131 (30.75%) were overweight while 228 (53.52%) had normal BMI. Amongst the participants who had PE, 48 (66.67%) had normal BMI, 16 (22.22%) were overweight while 8 (11.11%) were obese. Majority of participants (66.67%) with probable/borderline PE had normal BMI, 16.67% were overweight while 16.67% were obese. P value of less than 0.05 was significant. Conclusion: This study shows that premature ejaculation is common amongst all age group and has a variable relationship with body habitus, possibly dependent on the sub-type of premature ejaculation. There was an inverse correlation between PE and BMI in younger populations which suggests a lifelong sub-type. PE was also commoner in leaner younger participants and the number of participants with PE decreased as BMI increased.
VL - 9
IS - 1
ER -
Kenenna, O., Terkaa, A., Felix, M., Christopher, O., Sadiq, A. (2025). Premature Ejaculation: Prevalence and Relationship with Body Mass Index. International Journal of Clinical Urology, 9(1), 101-106. https://doi.org/10.11648/j.ijcu.20250901.27
Kenenna, O.; Terkaa, A.; Felix, M.; Christopher, O.; Sadiq, A. Premature Ejaculation: Prevalence and Relationship with Body Mass Index. Int. J. Clin. Urol.2025, 9(1), 101-106. doi: 10.11648/j.ijcu.20250901.27
Kenenna O, Terkaa A, Felix M, Christopher O, Sadiq A. Premature Ejaculation: Prevalence and Relationship with Body Mass Index. Int J Clin Urol. 2025;9(1):101-106. doi: 10.11648/j.ijcu.20250901.27
@article{10.11648/j.ijcu.20250901.27,
author = {Obiatuegwu Kenenna and Atim Terkaa and Magnus Felix and Otabor Christopher and Abu Sadiq},
title = {Premature Ejaculation: Prevalence and Relationship with Body Mass Index
},
journal = {International Journal of Clinical Urology},
volume = {9},
number = {1},
pages = {101-106},
doi = {10.11648/j.ijcu.20250901.27},
url = {https://doi.org/10.11648/j.ijcu.20250901.27},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcu.20250901.27},
abstract = {Introduction: Premature ejaculation is one of the major disorders of sexual functions in males. The prevalence rate of 25-40% has been reported across all age groups globally. Ejaculation latency is affected by psychosomatic factors which may include obesity but the relationship between PE and obesity have not been well documented in sub-Saharan Africa. This study evaluates the prevalence of PE and correlation between PE and body mass index. Methods: This is a prospective cross-sectional study carried out in Federal Capital Territory (FCT) Abuja, Nigeria over a period of 2 years from January 2019 to December 2020. By simple random sampling, participants were recruited for the study. Two questionnaires (a proforma and PEDT) were administered to all the participants who gave consent to be enrolled and met the inclusion criteria. Two basic anthropometric measurements (weight and height) were objectively obtained. Data obtained were analyzed using Statistical Package for Social Sciences version 20.0. P value of less than 0.05 was considered statistically significant. Results: A total of 426 persons participated in the study. Majority of the participants (51.88%) fell within the age range of 20-30 years, while seventy-five participants (17.61%) were between the age ranges of 31-40 years. Those that fell within the age range of 41-50, 51-60, and 61-70 years were 16.43%, 8.22% and 5.87% respectively. Seventy-two participants (16.9%) had PE while three hundred and six participants (71.83%) had no PE. Probable/borderline PE was noted in 48 (11.27%) participants. Mean age of participants with PE was 27.88 years while the mean age of participants with borderline PE was 25.67 years. Mean age of participants with no PE was 41.85 years. Sixty-seven participants (15.73%) were obese, 131 (30.75%) were overweight while 228 (53.52%) had normal BMI. Amongst the participants who had PE, 48 (66.67%) had normal BMI, 16 (22.22%) were overweight while 8 (11.11%) were obese. Majority of participants (66.67%) with probable/borderline PE had normal BMI, 16.67% were overweight while 16.67% were obese. P value of less than 0.05 was significant. Conclusion: This study shows that premature ejaculation is common amongst all age group and has a variable relationship with body habitus, possibly dependent on the sub-type of premature ejaculation. There was an inverse correlation between PE and BMI in younger populations which suggests a lifelong sub-type. PE was also commoner in leaner younger participants and the number of participants with PE decreased as BMI increased.
},
year = {2025}
}
TY - JOUR
T1 - Premature Ejaculation: Prevalence and Relationship with Body Mass Index
AU - Obiatuegwu Kenenna
AU - Atim Terkaa
AU - Magnus Felix
AU - Otabor Christopher
AU - Abu Sadiq
Y1 - 2025/06/20
PY - 2025
N1 - https://doi.org/10.11648/j.ijcu.20250901.27
DO - 10.11648/j.ijcu.20250901.27
T2 - International Journal of Clinical Urology
JF - International Journal of Clinical Urology
JO - International Journal of Clinical Urology
SP - 101
EP - 106
PB - Science Publishing Group
SN - 2640-1355
UR - https://doi.org/10.11648/j.ijcu.20250901.27
AB - Introduction: Premature ejaculation is one of the major disorders of sexual functions in males. The prevalence rate of 25-40% has been reported across all age groups globally. Ejaculation latency is affected by psychosomatic factors which may include obesity but the relationship between PE and obesity have not been well documented in sub-Saharan Africa. This study evaluates the prevalence of PE and correlation between PE and body mass index. Methods: This is a prospective cross-sectional study carried out in Federal Capital Territory (FCT) Abuja, Nigeria over a period of 2 years from January 2019 to December 2020. By simple random sampling, participants were recruited for the study. Two questionnaires (a proforma and PEDT) were administered to all the participants who gave consent to be enrolled and met the inclusion criteria. Two basic anthropometric measurements (weight and height) were objectively obtained. Data obtained were analyzed using Statistical Package for Social Sciences version 20.0. P value of less than 0.05 was considered statistically significant. Results: A total of 426 persons participated in the study. Majority of the participants (51.88%) fell within the age range of 20-30 years, while seventy-five participants (17.61%) were between the age ranges of 31-40 years. Those that fell within the age range of 41-50, 51-60, and 61-70 years were 16.43%, 8.22% and 5.87% respectively. Seventy-two participants (16.9%) had PE while three hundred and six participants (71.83%) had no PE. Probable/borderline PE was noted in 48 (11.27%) participants. Mean age of participants with PE was 27.88 years while the mean age of participants with borderline PE was 25.67 years. Mean age of participants with no PE was 41.85 years. Sixty-seven participants (15.73%) were obese, 131 (30.75%) were overweight while 228 (53.52%) had normal BMI. Amongst the participants who had PE, 48 (66.67%) had normal BMI, 16 (22.22%) were overweight while 8 (11.11%) were obese. Majority of participants (66.67%) with probable/borderline PE had normal BMI, 16.67% were overweight while 16.67% were obese. P value of less than 0.05 was significant. Conclusion: This study shows that premature ejaculation is common amongst all age group and has a variable relationship with body habitus, possibly dependent on the sub-type of premature ejaculation. There was an inverse correlation between PE and BMI in younger populations which suggests a lifelong sub-type. PE was also commoner in leaner younger participants and the number of participants with PE decreased as BMI increased.
VL - 9
IS - 1
ER -