Background & Aims: Remdesivir (REM) has been widely used to treat subjects affected by COVID-19 due to its broad-spectrum activity. The aim was to assess the REM effect on liver histopathology, enzymes, and alterations in oxidative stress markers. Methods: Forty-eight Wistar rats were separated into eight groups as follows: Group A (Control) received normal saline intraperitoneally (IP) for 10 days; Group B (Low-dose REM) received REM (2.8 mg/kg for the first day and 1.4 mg/kg for days 2 to 10, IP); Group C (High-dose REM) received REM (8.5 mg/kg IP for the first 17 days and days 2 to 10); Group D (High-dose REM+DEX (Dexamethasone)+ HEP (Heparin) received DEX (7 mg/kg intramuscularly for 10 days) and HEP (333 IU/kg subcutaneously on the first day and 250 IU/kg subcutaneously every 12 hours from day 2 to day 10); Group E (High-dose REM+ DEX); Group F (High-dose REM+ HEP); Group G (DEX); Group H (HEP). For statistical analysis, non-parametric tests (Kruskal-Wallis H and Mann-Whitney U) were used for pathological lesions (semi-quantitative data) between the different groups, and a p < 0.05 was considered significant. Results: There were mild to severe pathological changes in the treated groups, including cell swelling, vascular congestion. Also, the D and G groups showed similar pathological lesions, which were more severe than in other treated groups with a significant difference (p < 0.05). Conclusions: This study identified Remdesivir-induced liver toxicity and oxidative stress alterations in rats, underscoring the need for careful liver function monitoring, especially in patients with hepatic dysfunction. The findings recommend caution in using Remdesivir as a first-line treatment in such cases, and further studies are required to validate these effects and explore broader clinical implications.
| Published in | International Journal of Ecotoxicology and Ecobiology (Volume 9, Issue 4) |
| DOI | 10.11648/j.ijee.20240904.14 |
| Page(s) | 148-159 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Remdesivir, COVID-19, Liver Enzymes, Oxidative Stress
Parameters | Group A | Group B | Group C | Group D | Group E | Group F | Group G | Group H |
|---|---|---|---|---|---|---|---|---|
AST (U/L) | 119.83±34.55 | 143.5±34.87 | 152.67±12.82 | 150.75±27.32 | 138±16.82 | 158.8±23.34 | 133.75±13.75 | 134.17±14.84 |
ALT (U/L) | 87±18.89 | 89±21.62 | 87.33±12.72 | 103±8.17 | 112.33±7.51 | 83±17.18 | 124.5±59.12 | 86.83±21.36 |
ALP (U/L) | 245.33±70.36 | 248.67±75.21 | 190.67±86.73 | 171.5±44.28 | 171.67±17.9 | 137.2±11.95 | 175.5±75.19 | 266.17±95.29 |
LDH (IU/L) | 363.83±98.47 | 386±284.5 | 163.5±59.25 | 120.25±40.33 | 167.25±36.32 | 241.33±103.79 | 118.25±34.55a | 165.33±99.84 |
CK (U/L) | 235.17±89.27 | 193.67±143.2 | 113±24.32 | 70.25±20.78b | 115.5±65.22 | 175.5±61.12 | 94.75±22.41 | 114.83±59.15 |
Albumin (g/dL) | 2.22±1.08 | 2.93±1.06 | 2.27±0.31 | 2.67±0.12 | 2±1.14 | 1.94±0.92 | 1.82±0.62 | 2.47±0.58 |
Protein (g/dl) | 7.3±1.43 | 6.92±2.07 | 6.99±0.71 | 7.23±1.12 | 5±1.55 | 5.26±3.61 | 6.92±4.1 | 7.18±2.78 |
Parameters | Group A | Group B | Group C | Group D | Group E | Group F | Group G | Group H |
|---|---|---|---|---|---|---|---|---|
LiverTAC (ng/mL) | 353.86 ±27.7 | 377.39 ±54.37 | 458.73 ±67.84a | 346.63 ±34.39c | 364.58 ±26.4 | 498.82 ±37.99abde | 467.06 ±37.49ad | 472.71 ±84.06abde |
LiverSOD (U/mL) | 3.82±1.12 | 5.12±4.71 | 3.94±0.8 | 1.23±0.33 | 2.92±0.82 | 3.26±0.76 | 2.69±1.06 | 2.39±0.93 |
LiverGPx (pg/mL) | 10.89±1.86 | 15.53±2.25 | 14.46±2.86 | 30.26±6.36abc | 22.56±4.96a | 23.8±5.58ac | 21.73±7.06a | 26±3.17abc |
Livercatalase (U/gm) | 25.72±3.23 | 24.24±3.05 | 25.56±2.21 | 25.7±2.81 | 22.95±4.41 | 28.28±4.7 | 29.12±4.42 | 31.7±3.24be |
LiverMDA (µmol/l) | 7.3±1.13 | 3.82±0.8a | 2.39±0.84a | 3.12±0.52a | 5.69±0.67cd | 6.96±1.47bcd | 3.11±1.07aef | 3.64±0.35aef |
Groups | Cell swelling | Vascular congestion | Hepatocyte atrophy | Hepatocyte degeneration | Necrosis |
|---|---|---|---|---|---|
A* | 0** | 0 | 0 | 0 | 0 |
B | 0 | +1 | +1 | 0 | 0 |
C | 0 | +2 | +1 | +1 | +1 |
D | +2 | +2 | 0 | 0 | 0 |
E | +1 | +3 | 0 | +1 | 0 |
F | 0 | +1 | +1 | +1 | 0 |
G | +1 | +2 | 0 | 0 | 0 |
H | +1 | +1 | +1 | 0 | 0 |
REM | Remdesivir |
DEX | Dexamethasone |
HEP | Heparin |
IP | Intraperitoneally |
WHO | World Health Organization |
FDA | Food and Drug Administration |
COVID-19 | Coronavirus Disease 2019 |
SARS-CoV | Severe Acute Respiratory Syndrome Coronavirus |
DHEW | Department of Health, Education, and Welfare |
NIH | National Institutes of Health |
H&E | Hematoxylin and Eosin |
PBS | Phosphate Buffer Solution |
ANOVA | Analysis of Variance |
SPSS | Statistical Package for the Social Sciences |
AST | Aspartate Aminotransferase |
ALT | Alanine Transaminase |
ALP | Alkaline Phosphatases |
LDH | Lactate Dehydrogenase |
CK | Creatine Kinase |
TAC | Total Antioxidant Capacity |
SOD | Superoxide Dismutase |
GPx | Glutathione Peroxidase |
MDA | Malondialdehyde |
| [1] | Helmy YA, Fawzy M, Elaswad A, Sobieh A, Kenney SP, Shehata AA. The COVID-19 Pandemic: A Comprehensive Review of taxonomy, genetics, Epidemiology, diagnosis, Treatment, and control. Journal of Clinical Medicine. 2020; 9(4): 1225. |
| [2] | Weiss SR, Leibowitz JL. Coronavirus pathogenesis. In: Advances in Virus Research.; 2011: 85-164. |
| [3] | Lim YX, Ng YL, Tam JP, Liu DX. Human Coronaviruses: A Review of Virus–Host Interactions. Diseases. 2016; 4(4): 26. |
| [4] | Zhang Y, Geng X, Tan Y, et al. New understanding of the damage of SARS-CoV-2 infection outside the respiratory system. Biomedicine & Pharmacotherapy. 2020; 127: 110195. |
| [5] | Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel Coronavirus–Infected pneumonia in Wuhan, China. JAMA. 2020; 323(11): 1061. |
| [6] | Wen W, Chen C, Tang J, et al. Efficacy and safety of three new oral antiviral treatment (molnupiravir, fluvoxamine and Paxlovid) for COVID-19: a meta-analysis. Annals of Medicine. 2022; 54(1): 516-523. |
| [7] | Paranjpe I, Russak A, De Freitas JK, et al. Retrospective cohort study of clinical characteristics of 2199 hospitalised patients with COVID-19 in New York City. BMJ Open. 2020; 10(11): e040736. |
| [8] | Matos R, Chung KK. DoD COVID-19 Practice Management Guide: Clinical Management of COVID-19. Defense Health Agency Falls Church United States. Published online June 18, 2020. |
| [9] | Beigel JH, Tomashek KM, Dodd LE, et al. Remdesivir for the treatment of Covid-19 — Final report. The New England Journal of Medicine. 2020; 383(19): 1813-1826. |
| [10] | Pan L, Mu M, Yang PC, et al. Clinical characteristics of COVID-19 patients with digestive symptoms in Hubei, China: a descriptive, Cross-Sectional, multicenter study. The American Journal of Gastroenterology. 2020; 115(5): 766-773. |
| [11] | Lingas G, Néant N, Gaymard A, et al. Effect of remdesivir on viral dynamics in COVID-19 hospitalized patients: a modelling analysis of the randomized, controlled, open-label DisCoVeRy trial. Journal of Antimicrobial Chemotherapy. 2022; 77(5): 1404-1412. |
| [12] | Qiu M, Huang S, Luo C, et al. Pharmacological and clinical application of heparin progress: An essential drug for modern medicine. Biomedicine & Pharmacotherapy. 2021; 139: 111561. |
| [13] | Charan J, Kaur RJ, Bhardwaj P, et al. Rapid review of suspected adverse drug events due to remdesivir in the WHO database; findings and implications. Expert Review of Clinical Pharmacology. 2020; 14(1): 95-103. |
| [14] | Zampino R, Mele F, Florio LL, et al. Liver injury in remdesivir-treated COVID-19 patients. Hepatology International. 2020; 14(5): 881-883. |
| [15] | Ntyonga-Pono MP. COVID-19 infection and oxidative stress: an under-explored approach for prevention and treatment? The Pan African Medical Journal. 2020; 35 (Supp 2). |
| [16] | Cecchini R, Cecchini AL. SARS-CoV-2 infection pathogenesis is related to oxidative stress as a response to aggression. Medical Hypotheses. 2020; 143: 110102. |
| [17] | Li M, Zhu D, Yang J, et al. Clinical treatment experience in severe and critical COVID-19. Mediators of Inflammation. 2021; 1-8. |
| [18] | Alam MS, Czajkowsky DM. SARS-CoV-2 infection and oxidative stress: Pathophysiological insight into thrombosis and therapeutic opportunities. Cytokine & Growth Factor Reviews. 2022; 63: 44-57. |
| [19] | Xu L, Liu J, Lu M, Yang D, Zheng X. Liver injury during highly pathogenic human coronavirus infections. Liver International. 2020; 40(5): 998-1004. |
| [20] | Schönrich G, Raftery M, Samstag Y. Devilishly radical NETwork in COVID-19: Oxidative stress, neutrophil extracellular traps (NETs), and T cell suppression. Advances in Biological Regulation. 2020; 77: 100741. |
| [21] | Klopfleisch R. Multiparametric and semiquantitative scoring systems for the evaluation of mouse model histopathology - a systematic review. BMC Veterinary Research. 2013; 9(1): 123. |
| [22] | Van Laar SA, De Boer MGJ, Gombert-Handoko KB, Guchelaar H, Zwaveling J. Liver and kidney function in patients with Covid-19 treated with remdesivir. British Journal of Clinical Pharmacology. 2021; 87(11): 4450-4454. |
| [23] | Zhang Y, Zheng L, Liu L, Zhao M, Xiao J, Zhao Q. Liver impairment in COVID-19 patients: A retrospective analysis of 115 cases from a single centre in Wuhan city, China. Liver International. 2020; 40(9): 2095-2103. |
| [24] | Wang Y, Zhang D, Du G, et al. Remdesivir in adults with severe COVID-19: a randomised, double-blind, placebo-controlled, multicentre trial. The Lancet. 2020; 395(10236): 1569-1578. |
| [25] | Hariri BA, Barman M, Haider V, et al. Efficacy and Adverse Effects of Remdesivir in Patients with COVID-19 Pneumonia: A Retrospective Study. Research Square (Research Square). Published online April 10, 2023. |
| [26] | Lin K, Gausman V, Poles MA, Popov V. Acute liver failure secondary to remdesivir in the treatment of COVID-19. ACG Case Reports Journal. 2022; 9(10): e00866. |
| [27] | Goldman JD, Lye DC, Hui DSC, et al. Remdesivir for 5 or 10 Days in Patients with Severe Covid-19. The New England Journal of Medicine. 2020; 383(19): 1827-1837. |
| [28] | Kulkarni AV, Kumar P, Tevethia HV, et al. Systematic review with meta-analysis: liver manifestations and outcomes in COVID-19. Alimentary Pharmacology & Therapeutics. 2020; 52(4): 584-599. |
| [29] | Yadav DK, Singh A, Zhang Q, et al. Involvement of liver in COVID-19: systematic review and meta-analysis. Gut. 2020; 70(4): 807-809. |
| [30] | Kumar-M P, Mishra S, Jha DK, et al. Coronavirus disease (COVID-19) and the liver: a comprehensive systematic review and meta-analysis. Hepatology International. 2020; 14(5): 711-722. |
| [31] | Paliogiannis P, Zinellu A. Bilirubin levels in patients with mild and severe Covid-19: A pooled analysis. Liver International. 2020; 40(7): 1787-1788. |
| [32] | Golabi S, Ghasemi S, Adelipour M, et al. Oxidative Stress and Inflammatory Status in COVID-19 outpatients: A Health Center-Based Analytical Cross-Sectional Study. Antioxidants. 2022; 11(4): 606. |
| [33] | Martín-Fernández M, Aller R, Heredia-Rodríguez M, et al. Lipid peroxidation as a hallmark of severity in COVID-19 patients. Redox Biology. 2021; 48: 102181. |
| [34] | Lage SL, Amaral EP, Hilligan KL, et al. Persistent oxidative stress and inflammasome activation in CD14highCD16− monocytes from COVID-19 patients. Frontiers in Immunology. 2022; 12. |
| [35] | Yaghoubi N, Youssefi M, Azad FJ, Farzad F, Yavari Z, Avval FZ. Total antioxidant capacity as a marker of severity of COVID-19 infection: Possible prognostic and therapeutic clinical application. Journal of Medical Virology. 2021; 94(4): 1558-1565. |
APA Style
Abbasi, M. M., Darbani, R., Rabet, O., Ghorbanihaghjo, A., Rashtchizadeh, N., et al. (2024). Effects of Remdesivir on Liver Enzymes, Oxidative Stress and Liver Histopathology in Rats. International Journal of Ecotoxicology and Ecobiology, 9(4), 148-159. https://doi.org/10.11648/j.ijee.20240904.14
ACS Style
Abbasi, M. M.; Darbani, R.; Rabet, O.; Ghorbanihaghjo, A.; Rashtchizadeh, N., et al. Effects of Remdesivir on Liver Enzymes, Oxidative Stress and Liver Histopathology in Rats. Int. J. Ecotoxicol. Ecobiol. 2024, 9(4), 148-159. doi: 10.11648/j.ijee.20240904.14
AMA Style
Abbasi MM, Darbani R, Rabet O, Ghorbanihaghjo A, Rashtchizadeh N, et al. Effects of Remdesivir on Liver Enzymes, Oxidative Stress and Liver Histopathology in Rats. Int J Ecotoxicol Ecobiol. 2024;9(4):148-159. doi: 10.11648/j.ijee.20240904.14
@article{10.11648/j.ijee.20240904.14,
author = {Mehran Mesgari Abbasi and Roya Darbani and Oldouz Rabet and Amir Ghorbanihaghjo and Nadereh Rashtchizadeh and Sina Raeisi and Monireh Khordadmehr},
title = {Effects of Remdesivir on Liver Enzymes, Oxidative Stress and Liver Histopathology in Rats
},
journal = {International Journal of Ecotoxicology and Ecobiology},
volume = {9},
number = {4},
pages = {148-159},
doi = {10.11648/j.ijee.20240904.14},
url = {https://doi.org/10.11648/j.ijee.20240904.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijee.20240904.14},
abstract = {Background & Aims: Remdesivir (REM) has been widely used to treat subjects affected by COVID-19 due to its broad-spectrum activity. The aim was to assess the REM effect on liver histopathology, enzymes, and alterations in oxidative stress markers. Methods: Forty-eight Wistar rats were separated into eight groups as follows: Group A (Control) received normal saline intraperitoneally (IP) for 10 days; Group B (Low-dose REM) received REM (2.8 mg/kg for the first day and 1.4 mg/kg for days 2 to 10, IP); Group C (High-dose REM) received REM (8.5 mg/kg IP for the first 17 days and days 2 to 10); Group D (High-dose REM+DEX (Dexamethasone)+ HEP (Heparin) received DEX (7 mg/kg intramuscularly for 10 days) and HEP (333 IU/kg subcutaneously on the first day and 250 IU/kg subcutaneously every 12 hours from day 2 to day 10); Group E (High-dose REM+ DEX); Group F (High-dose REM+ HEP); Group G (DEX); Group H (HEP). For statistical analysis, non-parametric tests (Kruskal-Wallis H and Mann-Whitney U) were used for pathological lesions (semi-quantitative data) between the different groups, and a p Results: There were mild to severe pathological changes in the treated groups, including cell swelling, vascular congestion. Also, the D and G groups showed similar pathological lesions, which were more severe than in other treated groups with a significant difference (p < 0.05). Conclusions: This study identified Remdesivir-induced liver toxicity and oxidative stress alterations in rats, underscoring the need for careful liver function monitoring, especially in patients with hepatic dysfunction. The findings recommend caution in using Remdesivir as a first-line treatment in such cases, and further studies are required to validate these effects and explore broader clinical implications.
},
year = {2024}
}
TY - JOUR T1 - Effects of Remdesivir on Liver Enzymes, Oxidative Stress and Liver Histopathology in Rats AU - Mehran Mesgari Abbasi AU - Roya Darbani AU - Oldouz Rabet AU - Amir Ghorbanihaghjo AU - Nadereh Rashtchizadeh AU - Sina Raeisi AU - Monireh Khordadmehr Y1 - 2024/11/22 PY - 2024 N1 - https://doi.org/10.11648/j.ijee.20240904.14 DO - 10.11648/j.ijee.20240904.14 T2 - International Journal of Ecotoxicology and Ecobiology JF - International Journal of Ecotoxicology and Ecobiology JO - International Journal of Ecotoxicology and Ecobiology SP - 148 EP - 159 PB - Science Publishing Group SN - 2575-1735 UR - https://doi.org/10.11648/j.ijee.20240904.14 AB - Background & Aims: Remdesivir (REM) has been widely used to treat subjects affected by COVID-19 due to its broad-spectrum activity. The aim was to assess the REM effect on liver histopathology, enzymes, and alterations in oxidative stress markers. Methods: Forty-eight Wistar rats were separated into eight groups as follows: Group A (Control) received normal saline intraperitoneally (IP) for 10 days; Group B (Low-dose REM) received REM (2.8 mg/kg for the first day and 1.4 mg/kg for days 2 to 10, IP); Group C (High-dose REM) received REM (8.5 mg/kg IP for the first 17 days and days 2 to 10); Group D (High-dose REM+DEX (Dexamethasone)+ HEP (Heparin) received DEX (7 mg/kg intramuscularly for 10 days) and HEP (333 IU/kg subcutaneously on the first day and 250 IU/kg subcutaneously every 12 hours from day 2 to day 10); Group E (High-dose REM+ DEX); Group F (High-dose REM+ HEP); Group G (DEX); Group H (HEP). For statistical analysis, non-parametric tests (Kruskal-Wallis H and Mann-Whitney U) were used for pathological lesions (semi-quantitative data) between the different groups, and a p Results: There were mild to severe pathological changes in the treated groups, including cell swelling, vascular congestion. Also, the D and G groups showed similar pathological lesions, which were more severe than in other treated groups with a significant difference (p < 0.05). Conclusions: This study identified Remdesivir-induced liver toxicity and oxidative stress alterations in rats, underscoring the need for careful liver function monitoring, especially in patients with hepatic dysfunction. The findings recommend caution in using Remdesivir as a first-line treatment in such cases, and further studies are required to validate these effects and explore broader clinical implications. VL - 9 IS - 4 ER -
Drug Applied Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
Drug Applied Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
Drug Applied Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
Department of Clinical Biochemistry and Laboratory Medicine, Tabriz University of Medical Sciences, Tabriz, Iran
Biotechnology Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
Pediatric Health Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
Department of Pathobiology, Faculty of Veterinary Medicine, University of Tabriz, Tabriz, Iran
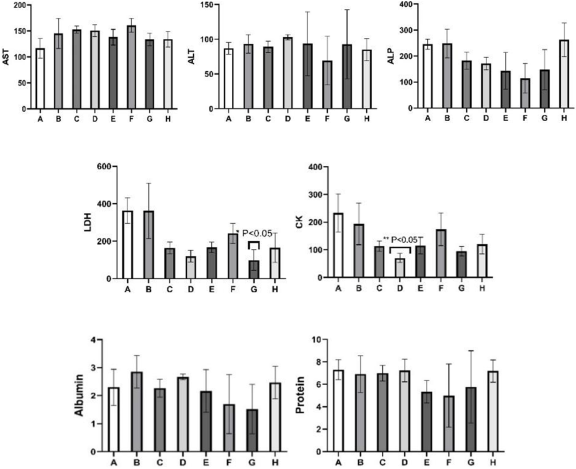
Figure 1. The data of AST, ALT, ALP, LDH, CK, Albumin, and Protein levels of the study groups.Figure 2 shows the correlations between the biochemistry parameters. As shown in Figure 2 H, I, and J, Liver ALT level was negatively correlated with liver ALP level (r = − 0.305, p = 0.041), CK level (r = − 0.395, p = 0.007), and LDH level (r = = − 0.353, p = 0.017). Also, liver AST level was negatively correlated with CK level (r = − 0.389, p = 0.008) (Figure 2 O). Also, liver AST level was negatively correlated with LDH level (r = − 0.401, p = 0.006) (Figure 2 P). Also, liver CK level was positively correlated with LDH level (r = − 0.871, P<0.001) (Figure 2 U).
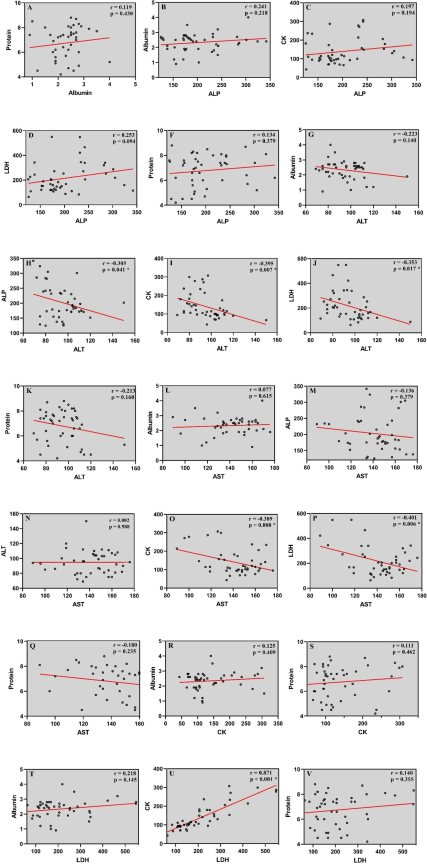
Figure 2. Shows the correlations between the biochemistry parameters. As shown in Figure 2 H, I, and J, liver ALT level was negatively correlated with liver ALP level (r = − 0.305, p = 0.041), CK level (r = − 0.395, p = 0.007) and LDH level (r = = − 0.353, p = 0.017). Also, liver AST level was negatively correlated with CK level (r = − 0.389, p = 0.008) (Figure 2 O). Also, liver AST level was negatively correlated with LDH level (r = − 0.401, p = 0.006) (Figure 2 P). Also, liver CK level was positively correlated with LDH level (r = − 0.871, P<0.001) (Figure 2 U).
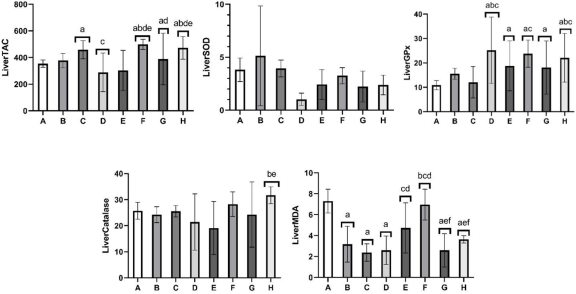
Figure 3. The data of liverTAC, SOD, GPx, Catalase, and MDA levels of the study groups.
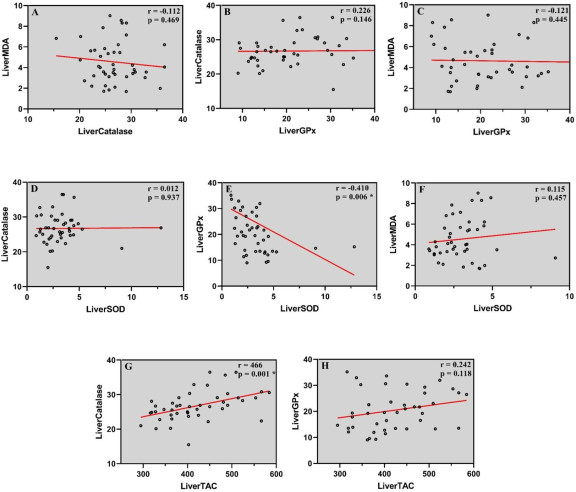
Figure 4. Shows the correlations between the Oxidative stress parameters. As shown in Figure 4 E, liver GPx level was negatively correlated with liver SOD level (r = − 0.410, p = 0.006). Also, liver catalase level was positively correlated with liver TAC level (r = 0.466, p = 0.001) (Figure 4 G).
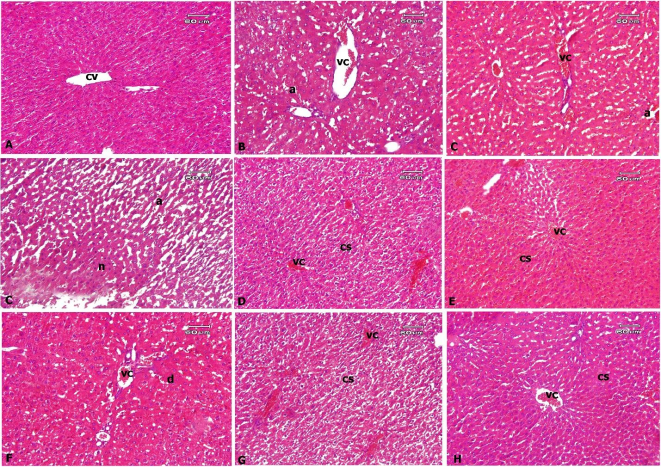
Figure 5. Liver, rat. A: normal control group with a normal construction of central vein (cv) and hepatocytes. B: Low-dose Rem; C: High-dose Rem; D: Rem + Dex + Hep; E: Rem + Dex; F: Rem + Hep; G: Dex; H: Hep. There were vascular congestion (vc) in all treated groups with severe grade in the E group, moderate grade in the C, D, and G groups, and mild grade in the B, F, and H groups. Of note, the C group presented mild focal necrosis (n) associated with mild hepatocyte atrophy (a). However, hepatocyte atrophy (a), degeneration (d), and cell swelling (cs) were observed in most groups. H&E.
Information

