Abstract
Background and Objectives: Acute Kidney Injury (AKI) in cirrhosis is a major determinant of morbidity and mortality. This study aims to assess the proportion, common predisposing factors and the mortality rate of hospitalised patients with AKI and cirrhosis. Methods: A single-center, longitudinal study was done in our setting including 186 patients with cirrhosis hospitalized to ward or ICU. AKI was diagnosed and staged as per ICA-AKI criteria. The proportion of AKI was calculated in percentage. Risk factors for AKI were recorded and their association was tested by chi-square test. Patient outcome (in terms of survived or deceased) was recorded and mortality rate was calculated in terms of percentage. Results: Proportion of AKI in hospitalized patients with cirrhosis was 39.7% (74/186). Alcoholic liver disease, NAFLD & hepatitis-B related cirrhosis comprised more than 90% of cirrhosis. Most patients with AKI had advanced stages of cirrhosis (CTP-A: 8, CTP-B: 18, CTP-C: 48). The common predisposing factors for AKI in cirrhotic patients were variceal bleeding (44.6%) and SBP (29.7%), while less common risk factors were infections like UTI (7%), LRTI (4%) and cellulitis (1.4%), along with large volume paracentesis (9.5%), recent over diuresis (8%), nephrotoxic drug intake (2.7%) and dehydration (1.4%). Most of the patients with cirrhosis who developed AKI had early stages of AKI. The mortality rate among hospitalized patients with cirrhosis and AKI was 32.4%. AKI was found to have a significant association with patient’s survival in cirrhosis. Conclusion: Burden of AKI, in terms of prevalence, morbidity as well as mortality among hospitalized patients with cirrhosis is significantly high in our region. Patients with definite predisposing factors require close monitoring for early detection of renal impairment.
|
Published in
|
International Journal of Gastroenterology (Volume 9, Issue 1)
|
|
DOI
|
10.11648/j.ijg.20250901.18
|
|
Page(s)
|
45-53 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2025. Published by Science Publishing Group
|
Keywords
Acute Kidney Injury, Cirrhosis, Proportion, Risk Factors, Mortality
1. Background
Cirrhosis is a complex disease process that leads to substantial volume shifts and increased vasodilation resulting in significant morbidity and mortality. Renal dysfunction adds to further complexity in cirrhosis contributing to worsened prognosis
| [1] | Ginès P, Schrier RW. Renal failure in cirrhosis. N Engl J Med. 2009; 361(13): 1279-90. |
[1]
. Pre-renal acute kidney injury (AKI) is the commonest cause of AKI in cirrhosis and majority of them are responsive to volume challenge. Hepato-renal syndrome (HRS) is the severe and volume unresponsive form of pre-renal AKI
| [2] | Wong F, Nadim MK, Kellum JA, Salerno F, Bellomo R, Gerbes A, et al. Working Party proposal for a revised classification system of renal dysfunction in patients with cirrhosis. Gut. 2011; 60(5): 702-9. |
[2]
. Model of End-stage Liver Disease (MELD) score is a strong predictor of 3-month mortality in patients with cirrhosis and it is also used to prioritize cirrhotic patients for orthotopic liver transplantation
| [3] | Wiesner R, Edwards E, Freeman R, Harper A, Kim R, Kamath P, et al; United Network for Organ Sharing Liver Disease Severity Score Committee. Model for end-stage liver disease (MELD) and allocation of donor livers. Gastroenterology. 2003; 124(1): 91-6. |
[3]
. As cirrhosis advances, underlying portal hypertension causes profound hemodynamic derangement, which in turn leads to marked splanchnic vasodilation. As a result, both renin-angiotensin-aldosterone system and the sympathetic nervous system gets activated, leading to intense renal vasoconstriction, which then plays a major role in the pathogenesis of ascites, hepato-renal syndrome and hyponatremia
| [4] | Ginès P, Guevara M, Arroyo V, Rodés J. Hepatorenal syndrome. Lancet. 2003; 362(9398): 1819-27. |
[4]
.
Table 1.
Staging of AKI according to International Club of Ascites criteria | [5] | Angeli P, Gines P, Wong F, Bernardi M, Boyer TD, Gerbes A, et al; International Club of Ascites. Diagnosis and management of acute kidney injury in patients with cirrhosis: revised consensus recommendations of the International Club of Ascites. Gut. 2015; 64(4): 531-7. |
Stage 1 | Increase in serum creatinine ≥0.3 mg/dl or ≥1.5-fold to 2-fold from baseline |
Stage 2 | Increase in serum creatinine > 2-fold to 3-fold from baseline |
Stage 3 | Increase of serum creatinine >3-fold from baseline or Increase in serum creatinine to ≥ 4 mg/dl with an acute increase by ≥0.3 mg/dl (or) Need for renal replacement therapy (RRT) |
As per the revised definition of AKI by International Club of Ascites (ICA) in 2015, increase in serum creatinine ≥ 0.3 mg/dl within 48 hours or a percentage increase of serum creatinine ≥ 50% from baseline which is known, or presumed, to have occurred within the prior 7 days defines AKI in cirrhosis. ICA has also revised the staging (
Table 1) and treatment response (
Table 2) of AKI in cirrhosis
| [5] | Angeli P, Gines P, Wong F, Bernardi M, Boyer TD, Gerbes A, et al; International Club of Ascites. Diagnosis and management of acute kidney injury in patients with cirrhosis: revised consensus recommendations of the International Club of Ascites. Gut. 2015; 64(4): 531-7. |
[5]
. In a cirrhotic patient with renal impairment, the crucial task is to identify the antecedent event that precipitated the renal failure. After ruling out the possibility of intrinsic renal disease, albumin infusion should be initiated which can improve the effective arterial blood volume, along with its antioxidant as well as anti-inflammatory properties
| [6] | Garcia-Martinez R, Noiret L, Sen S, Mookerjee R, Jalan R. Albumin infusion improves renal blood flow autoregulation in patients with acute decompensation of cirrhosis and acute kidney injury. Liver Int. 2015; 35(2): 335-43. |
| [7] | Wong F. Drug insight: the role of albumin in the management of chronic liver disease. Nat Clin Pract Gastroenterol Hepatol. 2007; 4(1): 43-51. |
[6, 7]
. Inadequate response to albumin infusion after 48 hours of infusion or advanced stages of AKI recommends vasoconstrictors like Terlipressin, Norepinephrine or combination of Octreotide and Midodrine
| [8] | Gupta K, Bhurwal A, Law C, Ventre S, Minacapelli CD, Kabaria S, et al. Acute kidney injury and hepatorenal syndrome in cirrhosis. World J Gastroenterol. 2021; 27(26): 3984-4003. |
[8]
.
Table 2.
Treatment response to AKI - International Club of Ascites criteria (2015) | [5] | Angeli P, Gines P, Wong F, Bernardi M, Boyer TD, Gerbes A, et al; International Club of Ascites. Diagnosis and management of acute kidney injury in patients with cirrhosis: revised consensus recommendations of the International Club of Ascites. Gut. 2015; 64(4): 531-7. |
No Response | No regression of AKI |
Partial Response | Regression of AKI stage with reduction of serum creatinine ≥ 0.3 mg/dl above baseline |
Complete Response | Regression of AKI stage with reduction of serum creatinine to a value within 0.3 mg/dl of baseline |
In the Indian context, various retrospective studies have been conducted in the past, but prospective studies, especially based on ICA-AKI criteria (2015), on AKI in cirrhosis are limited. Early identification of predisposing factors for AKI and immediate treatment at the onset is essential for a better prognosis in patients with cirrhosis.
2. Aim
(1) To study the proportion of AKI among hospitalized patients with Cirrhosis.
(2) To study the predisposing factors for AKI in cirrhosis.
(3) To study the mortality rate in cirrhotic patients with AKI during hospital stay.
3. Methodology
3.1. Design and Patients
This is an observational, prospective, longitudinal study where 186 patients admitted to IP department (ward and ICU) of the Department of Gastroenterology, Government Medical College, Kozhikode with a diagnosis of chronic liver disease over the period of one year (September 2020 - August 2021) were randomly selected and studied. Eligible patients were hospitalized patients aged ≥18 years with a known diagnosis of cirrhosis. Exclusion criteria included patients with prior kidney or liver transplant, patients with known underlying chronic kidney disease, patients with obstructive uropathy and pregnant females.
3.2. Methods
Hospitalized patients with cirrhosis were randomly selected. Detailed clinical history along with clinical examination were done at the time of admission. Major clinical events, including decompensation, were carefully evaluated and appropriate investigations were performed. Cirrhosis was staged based on Child-Turcotte-Pugh (CTP) classification and MELD scoring was also done. Etiology of cirrhosis was also determined based on history, biochemical and serological investigations along with liver biopsy (if needed). AKI in cirrhosis was defined based on revised ICA-AKI criteria (2015). The proportion of AKI in hospitalized cirrhotic patients was calculated. Predisposing factors for AKI in cirrhosis were analyzed based on clinical and laboratory evaluation and association in patients with and without AKI were studied. Baseline creatinine in the prior 3 months was collected. Serum Creatinine was measured at admission & subsequently monitored, until the discharge or death of patient. During hospitalization, peak serum creatinine value was noted and staging of AKI was done as per ICA-AKI criteria. All hospitalized patients with cirrhosis and AKI were managed as per the standard treatment guidelines, including the tackling of predisposing factors. Mortality rates in cirrhotic patients with and without AKI during hospital stay were measured as secondary objective.
3.3. Statistical Analysis
Statistical Analysis was done using SPSS 16 software. Patient characteristics were described with absolute frequencies, percentages and medians. The proportion of AKI in cirrhosis was analyzed as percentages. The risk factors for development of AKI in cirrhosis were evaluated by univariate analysis using chi-square test for categorical variables and univariate logistic regression for continuous variables (like Age & MELD score). The risk factors which were found to be significant in univariate analysis were taken into multivariate analysis using multiple logistic regression. Receiver Operating Characteristic (ROC) curve was used to evaluate the diagnostic capability of MELD score on AKI in cirrhosis. Mortality rates in cirrhotic patients with AKI also was analyzed as percentages. Comparison of MELD score among treatment response groups was done using ANOVA and post-hoc dunnet t-test.
4. Results
A total of 186 hospitalized patients with cirrhosis were enrolled in the study over a period of 1 year. 74 out of 186 patients with cirrhosis developed AKI, either at admission or during hospital stay. The proportion of AKI in hospitalized patients with cirrhosis is 39.7%. The demographic and clinical characteristics of cirrhotic patients with and without AKI are summarized in
Table 3. The mean age of patients with cirrhosis who developed AKI (57.9 ±12.95 years) was higher than those without AKI (50.65 ± 13.04 years). Our study population showed male predominance (61.3%) and among patients who developed AKI (n=74), 45 (60.8%) were males and 29 (39.2%) were females. Most patients who developed AKI had advanced underlying cirrhosis, of which 48 patients had CTP-C and 18 patients had CTP-B stages out of 74 patients. Among patients without AKI, CTP-A and CTP-B (102 out of 112 patients) stages of underlying cirrhosis predominated. The mean MELD score of cirrhotic patients was higher among patients with AKI (26.97 ± 6.93) than those without AKI (15.44 ± 6). The utility of MELD score as a diagnostic marker for AKI in cirrhosis was evaluated using a receiver operating characteristic curve (ROC). The area under the curve was 0.888, indicating it is a fairly good marker bordering on excellent. Most common etiologies of cirrhosis in our study population were alcoholic liver disease (77 of 186 patients; 43.2%) followed by Non-Alcoholic Fatty Liver Disease (NAFLD) (51 of 186 patients; 37.8%), while HBV infection (11.3%), HCV infection (4.8%), autoimmune hepatitis (3.7%), Budd Chiari syndrome (3.2%) andWilson’s disease (1.6%) constitutes minor population. 6.4% of patients were cryptogenic. In patients with NAFLD related cirrhosis, more than 50% (28 of 51 patients) developed AKI, while none of the patients with budd chiari syndrome and autoimmune hepatitis developed AKI in our study.
Table 3. Demographic and clinical characteristics of the participants in the study.
Characteristics (N=186) | Cirrhosis with AKI (N=74) | Cirrhosis without AKI (N=112) |
Age* | 57.9 (12.95) | 50.65 (13.04) |
Male | 45 | 69 |
Female | 29 | 43 |
Child-Turcotte-Pugh (CTP) score |
CTP - A | 8 | 57 |
CTP – B | 18 | 45 |
CTP - C | 48 | 10 |
Model for end stage liver disease (MELD)* | 26.97 (6.93) | 15.44 (6) |
Previous decompensation | 62 | 49 |
Etiology of CLD |
Alcoholic liver disease | 32 | 45 |
NAFLD | 28 | 23 |
HBV | 10 | 11 |
HCV | 1 | 8 |
Wilson’s disease | 0 | 3 |
Autoimmune Hepatitis | 0 | 7 |
Budd chiari syndrome | 1 | 5 |
Cryptogenic | 2 | 10 |
4.1. Analysis of Risk Factors Associated with AKI in Cirrhotic Patients (Table 4) Table 4. Univariate analysis of risk factors for AKI in cirrhosis.
Risk factors | Odds ratio | 95% Confidence Interval | p value |
Variceal bleeding | 2.801 | 1.479 – 5.305 | 0.002 |
SBP | 2.962 | 1.399 – 6.268 | 0.005 |
Recent LVP | 5.746 | 1.160 – 28.477 | 0.031 |
Hyponatremia | 15.117 | 7.318 – 31.227 | < 0.001 |
Hepatic encephalopathy | 13.256 | 6.279 – 27.985 | < 0.001 |
As evaluated using univariate logistic regression, age (Odds Ratio [OR]-1.04; 95% Confidence Interval [CI]: 1.02-1.07) and MELD score (OR: 1.26; 95% CI: 1.18-1.34) were found to be significant risk factors for AKI in cirrhosis, while gender distribution had no significant association (OR: 1.03; 95% CI: 0.57 – 1.89). CTP score of underlying cirrhosis also had significant association with AKI (χ2 = 68.50, p < 0.001), as 82.8% of advanced CTP stage-C cirrhosis developed AKI in our study.
Common predisposing factors for AKI in cirrhosis seen in our study were variceal bleeding (44.6%), Spontaneous Bacterial Peritonitis (SBP) (29.7%), recent large volume paracentesis (LVP) (9.4%), recent history of over-diuresis (8%) and Urinary Tract Infection (UTI) (6.7%), while Non-Steroid Anti-Inflammatory Drugs (NSAID) use (2.7%), diarrhea (1.3%) and other infections like lower respiratory tract infection (LRTI), cellulitis and cholecystitis comprised only minority (< 5%). AKI was found to be associated with 56.9% of patients with variceal bleeding, 61.1% of patients with SBP, 77.8% of recent LVP, 100% of recent over diuresis. Hence, onset of AKI in cirrhosis was found to have significant statistical correlation with variceal bleeding (χ2 = 10.30, p=0.002), SBP (χ2 = 8.47, p=0.005), recent LVP (χ2 = 5.70, p=0.031) and recent history of over diuresis (χ2 = 9.38, p=0.003). Other infections like UTI, LRTI, cellulitis and cholecystitis were not found to have any statistical association with AKI in cirrhosis. Statistical significance was not tested with risk factors like diarrhea and recent intake of NSAID or any other nephrotoxic drug, as sufficient participants were not available for the analysis in our study, even though all 2 patients with NSAID intake and 1 out of 2 patients with diarrhea had associated AKI.
Among our cirrhotic patients, 75.3% of patients with hyponatremia and 78.3% of patients with hepatic encephalopathy had AKI. Significant statistical correlation was also established between AKI and hyponatremia (χ2 = 63.42, p< 0.001) as well as hepatic encephalopathy (χ2 = 54.94, p< 0.001).
After univariate analysis, the above-mentioned risk factors were taken into multivariate analysis using multiple logistic regression which has a very good predictive capability (Cox & Snell R-square – 0.434). In the multivariate analysis, MELD score (OR: 1.17; 95% CI:1.07 – 1.28) and variceal bleeding (OR: 4.16; 95% CI:1.49 – 11.63) were found to be significant risk factors for AKI when adjusted for other confounding factors (
Table 5).
Table 5. Multivariate analysis of risk factors for AKI in cirrhosis.
Risk factors | Odds ratio | 95% Confidence Interval | p value |
Age | 1.001 | 0.966 – 1.036 | 0.965 |
MELD score | 1.172 | 1.072 – 1.282 | < 0.001 |
Variceal bleed | 4.165 | 1.491 – 11.635 | 0.006 |
SBP | 2.383 | 0.80 – 7.098 | 0.119 |
Recent LVP | 3.636 | 0.504 – 26.214 | 0.20 |
Hepatic Encephalopathy | 1.891 | 0.605 – 5.907 | 0.273 |
Hyponatremia | 1.754 | 0.499 – 6.171 | 0.381 |
The factors identified as significant in univariate analysis were entered into a multivariate logistic regression model as predictors of acute kidney injury.
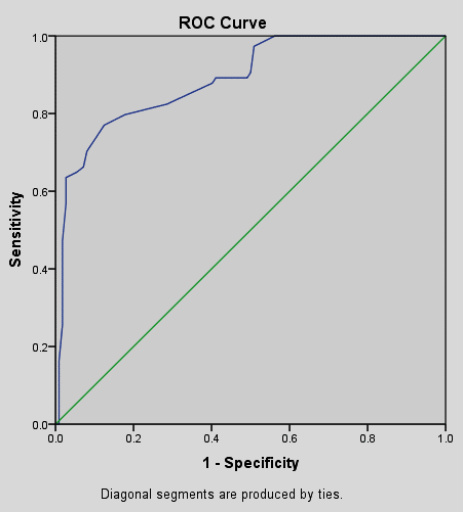
MELD score was evaluated as diagnostic marker of AKI using receiver operating characteristic curve (ROC). MELD score of 20 offered approximately 80% sensitivity and specificity. AUROC of 0.888 indicated a fairly good marker bordering on excellent (
Figure 2).
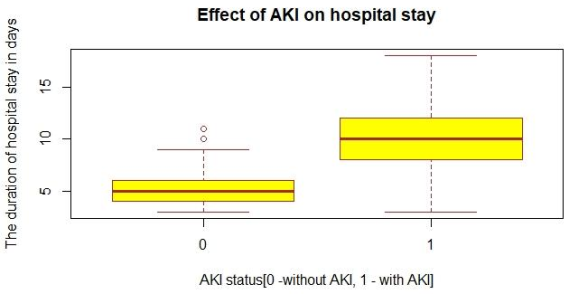
Figure 1. Boxplot comparing duration of hospital stay in patients with and without AKI.
(0 = Patients without AKI, 1 = Patients with AKI)
*The outliers in group 0 is shown with the serial number of data points
Figure 2. The Receiver Operating Characteristic (ROC) curve showing the predictive capability of Model for end stage liver disease (MELD) score as a diagnostic tool for acute kidney injury in liver cirrhosis.
4.2. Influence of AKI on Morbidity and Mortality of Patients with Cirrhosis
34 patients (18.3%) succumbed to their ailment, among which 24 had concurrent AKI and 10 patients had no associated AKI. Among patients with cirrhosis and AKI, 32.4% of patients succumbed to their illness. Therefore, AKI was found to be significantly associated with patient mortality in our study (OR – 4.89, 95% CI: 2.17-11.02).
Out of 59 patients (31.7%) who required ICU care during hospitalization, 83% (n=49) had AKI. 66.2% of patients with cirrhosis and AKI required ICU monitoring and a significant statistical association was also seen between AKI and ICU requirement (OR – 19.99, 95% CI: 8.91 - 44.88). The mean duration of hospitalization in patients with cirrhosis who developed AKI (9.92 ± 3.157 days) was found to be higher than those without AKI (5.07 ± 1.587 days) (
Figure 1).
Association between number of hospital days and MELD score was evaluated using simple linear regression and it was found that MELD score was a significant predictor for duration of hospital stay in our study population (R squared = 0.492).
4.3. Distribution & Influence of Peak Stages of AKI in Patients with Cirrhosis
Out of 74 patients with AKI in cirrhosis, stage-1 AKI (43.2% [n=32]) predominated, followed by stage-2 AKI (32.4% [n=24]) and stage-3 AKI (24.3% [n=18]).
Among the deceased patients with AKI and cirrhosis, the majority belonged to peak stage-3 AKI (66.7%) followed by stage-2 AKI (29.2%). Hence, the peak AKI stage has significant association with mortality in patients with cirrhosis and AKI (χ2 = 38.84, df = 2, p < 0.001). Advanced stages of AKI (stages 2 & 3) also had major ICU requirement (85%) and hence, found to have significant statistical correlation (χ2 = 49.55, p < 0.001).
4.4. Time of Onset of AKI in Patients with Cirrhosis
Among patients with cirrhosis, 66.2% (n=49) had AKI at admission or within 24 hours of admission, while 33.8% (n=25) developed AKI later (after 24 hours of admission).
In our study, mortality in cirrhotic patients with early onset AKI (46.9% [n=23]) was higher when compared to patients with delayed onset AKI (4% [n=1]), which was found to be statistically significant (OR: 0.047; 95% CI: 0.006-0.376).
4.5. Treatment Response in Patients with Cirrhosis
In our study, among patients with cirrhosis and AKI, 59.4% (n=44) had complete response, 23% (n=17) had partial response and 17.6% (n=13) had no response.
All patients with cirrhosis and AKI with no response to treatment had 100% mortality and survival was abysmal in partial responders also (10 of 17 patients; 58.8% mortality). Only 1 patient (2.3%) among complete responders didn’t survive. Treatment response in AKI had significant statistical association with mortality of cirrhotic patients (χ2 = 50.75, p < 0.001).
The mean duration of hospital stay among complete responders was 8.9 days (SD-2.5) and in partial responders was 10.1 days (SD-3.4), while non-responders had relatively higher duration of hospital stay of 12.8 days (SD-3.2). Duration of hospital stay was found to significantly differ according to responder status of patients (F=9.304; p<0.001). Post-hoc comparison using dunnett t-test showed that duration of hospital stay was found to significantly differ between non-responder and complete responders (p<0.001).
4.6. Renal Replacement Therapy (RRT)
13.5% (n=10) of patients with AKI and cirrhosis, who had stage-3 AKI, received RRT in our study and none of them survived.
5. Discussion
A longitudinal study was conducted on randomly selected 186 hospitalized patients with cirrhosis. 74 out of 186 patients developed AKI and the proportion of AKI in hospitalized patients with cirrhosis in our study is 39.78%. Western data had pointed out a significant burden of AKI in cirrhotic patients. Earlier in 2001, retrospective study by
Hampel H et al showed that 24.7% patients developed AKI within 15 days of hospitalization
| [9] | Hampel H, Bynum GD, Zamora E, El-Serag HB. Risk factors for the development of renal dysfunction in hospitalized patients with cirrhosis. Am J Gastroenterol. 2001; 96(7): 2206-10. |
[9]
. Later in 2013, a prospective study by
Fagundes C et al showed a very high proportion of 47% developing AKI (as per AKIN criteria) in hospitalized patients with cirrhosis
| [10] | Fagundes C, Barreto R, Guevara M, Garcia E, Solà E, Rodríguez E, et al. A modified acute kidney injury classification for diagnosis and risk stratification of impairment of kidney function in cirrhosis. J Hepatol. 2013; 59(3): 474-81. |
[10]
. According to the Indian data, a retrospective study by
Shetty S et al in 2018 showed that prevalence of AKI in hospitalized patients with cirrhosis was 35%
| [11] | Shetty S, Nagaraju SP, Shenoy S, Attur RP, Rangaswamy D, Rao IR et al. Acute kidney injury in patients with cirrhosis of liver: Clinical profile and predictors of outcome. Indian J Gastroenterol. 2018; 37(3): 248–254. |
[11]
. In 2020, an observational study from North India by
Arora MS et al showed 40.6% patients with AKI in patients with decompensated cirrhosis
| [12] | Arora MS, Kaushik R, Ahmad S, Kaushik RM. Profile of Acute Kidney Injury in Patients with Decompensated Cirrhosis at a Tertiary-Care Center in Uttarakhand, India. Dig Dis. 2020; 38(4): 335-343. |
[12]
. Another prospective observational study by
Kumar U et al in 2020 showed that 28.4% patients with cirrhosis developed AKI
| [13] | Kumar U, Kumar R, Jha SK, Jha AK, Dayal VM, Kumar A. Short-term mortality in patients with cirrhosis of the liver and acute kidney injury: A prospective observational study. Indian J Gastroenterol. 2020; 39(5): 457-464. |
[13]
.
In our study, the mean age of patients with cirrhosis who developed AKI (57.9 ±12.95 years) was higher than those without AKI (50.65 ± 13.04 years) and age had significant association with AKI in cirrhosis. In 2018, study by
Shetty S et al showed mean age of 51.7 years for patients with cirrhosis and AKI
| [11] | Shetty S, Nagaraju SP, Shenoy S, Attur RP, Rangaswamy D, Rao IR et al. Acute kidney injury in patients with cirrhosis of liver: Clinical profile and predictors of outcome. Indian J Gastroenterol. 2018; 37(3): 248–254. |
[11]
, while mean age was 48 years as per study by
Kumar U et al | [13] | Kumar U, Kumar R, Jha SK, Jha AK, Dayal VM, Kumar A. Short-term mortality in patients with cirrhosis of the liver and acute kidney injury: A prospective observational study. Indian J Gastroenterol. 2020; 39(5): 457-464. |
[13]
. In another study by Arora MS et al in 2020, mean age of patients with cirrhosis with AKI (48.9 ±10.11 years) was lower than those without AKI (51.72 ± 12.01 years) and age had no association with development of AKI in cirrhosis
| [12] | Arora MS, Kaushik R, Ahmad S, Kaushik RM. Profile of Acute Kidney Injury in Patients with Decompensated Cirrhosis at a Tertiary-Care Center in Uttarakhand, India. Dig Dis. 2020; 38(4): 335-343. |
[12]
.
Male population was higher in our study and predominated in both the groups of cirrhotic patients with and without AKI. However, sex distribution had no significant association with AKI in cirrhosis. Studies by
Shetty S et al | [11] | Shetty S, Nagaraju SP, Shenoy S, Attur RP, Rangaswamy D, Rao IR et al. Acute kidney injury in patients with cirrhosis of liver: Clinical profile and predictors of outcome. Indian J Gastroenterol. 2018; 37(3): 248–254. |
[11]
and
Kumar U et al | [13] | Kumar U, Kumar R, Jha SK, Jha AK, Dayal VM, Kumar A. Short-term mortality in patients with cirrhosis of the liver and acute kidney injury: A prospective observational study. Indian J Gastroenterol. 2020; 39(5): 457-464. |
[13]
also showed predominantly males with AKI in cirrhosis.
In our study, large majority (> 80%) of patients with advanced cirrhosis (especially CTP - C) developed AKI. Hence, the risk of AKI is proportional with severity of the underlying cirrhosis.
Arora MS et al also showed that CTP score was significantly higher in patients with AKI, implying that severity of cirrhosis may contribute to development of AKI (
p < 0.05)
| [12] | Arora MS, Kaushik R, Ahmad S, Kaushik RM. Profile of Acute Kidney Injury in Patients with Decompensated Cirrhosis at a Tertiary-Care Center in Uttarakhand, India. Dig Dis. 2020; 38(4): 335-343. |
[12]
. However,
Tsien C D et al showed no significant difference in the CTP score between patients with AKI and without AKI
| [14] | Tsien CD, Rabie R, Wong F. Acute kidney injury in decompensated cirrhosis. Gut. 2013; 62(1): 131-7. |
[14]
.
In our study, the mean MELD score among patients with cirrhosis and AKI (26.97 ± 6.93) was higher than those without AKI (15.44 ± 6), which agrees with the study by
Arora MS et al which also showed higher mean MELD score in patients with cirrhosis and AKI (27.9 ± 8.5) than in those without AKI (15 ± 6.3)
| [12] | Arora MS, Kaushik R, Ahmad S, Kaushik RM. Profile of Acute Kidney Injury in Patients with Decompensated Cirrhosis at a Tertiary-Care Center in Uttarakhand, India. Dig Dis. 2020; 38(4): 335-343. |
[12]
. MELD score (OR: 1.258; 95% CI:1.182-1.339) was found to be a significant risk factor for AKI in cirrhosis and a score of 20 or more was shown to have 80% sensitivity and specificity as a diagnostic tool for AKI in cirrhosis (AUROC - 0.88).
Majority (> 90%) of patients in our study had alcoholic liver disease, NAFLD or Hepatitis-B related cirrhosis and thus, AKI predominated in these 3 etiological groups of cirrhosis. Unlike other etiologies, more than half the population of NALFD developed AKI in our study. Alcoholic liver disease predominated in other studies by
Shetty S et al | [11] | Shetty S, Nagaraju SP, Shenoy S, Attur RP, Rangaswamy D, Rao IR et al. Acute kidney injury in patients with cirrhosis of liver: Clinical profile and predictors of outcome. Indian J Gastroenterol. 2018; 37(3): 248–254. |
[11]
,
Arora M S et al | [12] | Arora MS, Kaushik R, Ahmad S, Kaushik RM. Profile of Acute Kidney Injury in Patients with Decompensated Cirrhosis at a Tertiary-Care Center in Uttarakhand, India. Dig Dis. 2020; 38(4): 335-343. |
[12]
and
Kumar U et al | [13] | Kumar U, Kumar R, Jha SK, Jha AK, Dayal VM, Kumar A. Short-term mortality in patients with cirrhosis of the liver and acute kidney injury: A prospective observational study. Indian J Gastroenterol. 2020; 39(5): 457-464. |
[13]
.
5.1. Predisposing Factors for AKI in Cirrhosis
In our study, variceal bleeding (44.6%) and SBP (29.7%) were the most common predisposing factors for AKI in cirrhosis, followed by large volume paracentesis (9.4%), recent over diuresis (8%), UTI (6.7%), while other infections, NSAID or nephrotoxic drug intake (2.7%) and diarrhea (1.3%) comprised only minority. Among these risk factors, variceal bleed, SBP, recent over diuresis and recent LVP were found to have significant association with the onset of AKI in cirrhosis. However, when these risk factors were subjected to multivariate analysis using multiple logistic regression, after adjusting for confounding factors, only variceal bleeding was found to be a significant risk factor for the development of AKI in cirrhosis. Since sufficient participants were not available for the analysis of risk factors like dehydration and recent NSAID use, its association with AKI could not be analysed, even though all patients with recent NSAID use had developed AKI. Other predisposing factors like UTI, LRTI, cellulitis and cholecystitis in cirrhosis were not found to have any significant association with AKI in our study.
In a study by
de Carvalho G C et al in 2012, bacterial infections and hypovolemia accounted for more than 70% of cases of renal failure in patients with decompensated end stage liver disease
| [15] | Carvalho GC, Regis Cde A, Kalil JR, Cerqueira LA, Barbosa DS, Motta MP, et al. Causes of renal failure in patients with decompensated cirrhosis and its impact in hospital mortality. Ann Hepatol. 2012; 11(1): 90-5. |
[15]
. In another study by
Tsien C D et al, the most common precipitants for AKI were bacterial infections (including SBP), followed by large volume paracentesis and increase in diuretic doses
| [14] | Tsien CD, Rabie R, Wong F. Acute kidney injury in decompensated cirrhosis. Gut. 2013; 62(1): 131-7. |
[14]
. As per Indian data,
Kumar U et al showed that infections and hypovolemia were the most common causes of AKI in cirrhosis
| [13] | Kumar U, Kumar R, Jha SK, Jha AK, Dayal VM, Kumar A. Short-term mortality in patients with cirrhosis of the liver and acute kidney injury: A prospective observational study. Indian J Gastroenterol. 2020; 39(5): 457-464. |
[13]
, while
Arora M S et al showed SBP, sepsis and shock as common risk factors for AKI
| [12] | Arora MS, Kaushik R, Ahmad S, Kaushik RM. Profile of Acute Kidney Injury in Patients with Decompensated Cirrhosis at a Tertiary-Care Center in Uttarakhand, India. Dig Dis. 2020; 38(4): 335-343. |
[12]
. In concordance with above studies, variceal bleed, SBP were risk factors having significant association with AKI in our study. However, on the contrary, other bacterial infections (except SBP) were not found to have any significant association with AKI in cirrhosis.
In our study, hyponatremia and hepatic encephalopathy were found to have significant association with AKI in cirrhosis.
Shetty S et al showed that a large proportion (85%) of patients with cirrhosis and AKI had hepatic encephalopathy
| [11] | Shetty S, Nagaraju SP, Shenoy S, Attur RP, Rangaswamy D, Rao IR et al. Acute kidney injury in patients with cirrhosis of liver: Clinical profile and predictors of outcome. Indian J Gastroenterol. 2018; 37(3): 248–254. |
[11]
.
Kumar U et al also showed similar association between AKI and hepatic encephalopathy in 21% of patients with decompensated cirrhosis, which had significant association with patient mortality
| [13] | Kumar U, Kumar R, Jha SK, Jha AK, Dayal VM, Kumar A. Short-term mortality in patients with cirrhosis of the liver and acute kidney injury: A prospective observational study. Indian J Gastroenterol. 2020; 39(5): 457-464. |
[13]
.
5.2. Influence of AKI on Mortality and Morbidity Indices of Cirrhosis
In our study, 32.4% (n=24) of patients with cirrhosis and AKI succumbed to their illness and AKI was found to have significant impact on patient’s survival. 66.2% of patients with cirrhosis and AKI required ICU monitoring indicating higher morbidity than those without AKI.
Scott R A et al showed that cirrhotic patients with AKI had higher mortality rate than those without AKI (31.8% vs 3.8%, p<0.001)
| [16] | Scott RA, Austin AS, Kolhe NV, McIntyre CW, Selby NM. Acute kidney injury is independently associated with death in patients with cirrhosis. Frontline Gastroenterol. 2013; 4(3): 191-197. |
[16]
. Indian data also agrees with relatively higher mortality rate among cirrhotic patients with AKI as per studies by
Shetty S et al (44.7%)
| [11] | Shetty S, Nagaraju SP, Shenoy S, Attur RP, Rangaswamy D, Rao IR et al. Acute kidney injury in patients with cirrhosis of liver: Clinical profile and predictors of outcome. Indian J Gastroenterol. 2018; 37(3): 248–254. |
[11]
,
Arora MS et al (33.8%)
| [12] | Arora MS, Kaushik R, Ahmad S, Kaushik RM. Profile of Acute Kidney Injury in Patients with Decompensated Cirrhosis at a Tertiary-Care Center in Uttarakhand, India. Dig Dis. 2020; 38(4): 335-343. |
[12]
and
Kumar U et al (26.68%)
| [13] | Kumar U, Kumar R, Jha SK, Jha AK, Dayal VM, Kumar A. Short-term mortality in patients with cirrhosis of the liver and acute kidney injury: A prospective observational study. Indian J Gastroenterol. 2020; 39(5): 457-464. |
[13]
.
Our study also showed relatively longer mean duration of hospital stay in cirrhotic patients with AKI (9.92 ± 3.157 days) than those without AKI (5.07 ± 1.587 days), which complies with the data by
Shetty S et al (mean duration: 11 days)
| [11] | Shetty S, Nagaraju SP, Shenoy S, Attur RP, Rangaswamy D, Rao IR et al. Acute kidney injury in patients with cirrhosis of liver: Clinical profile and predictors of outcome. Indian J Gastroenterol. 2018; 37(3): 248–254. |
[11]
and
Scott R A et al (16 days vs 6 days,
p < 0.01)
| [16] | Scott RA, Austin AS, Kolhe NV, McIntyre CW, Selby NM. Acute kidney injury is independently associated with death in patients with cirrhosis. Frontline Gastroenterol. 2013; 4(3): 191-197. |
[16]
.
5.3. Stages of AKI and Its Impact on Patients with Cirrhosis
Early stages of AKI predominated our study, with peak AKI stage 1 (43.2%) being more common followed by stage 2 AKI (32.4%) & stage 3 AKI (24.3%).
Arora MS et al also showed similarly higher proportion of early stages of AKI in cirrhosis that majority (stage 1: 77.4%, stage 2: 19.7%, stage 3: 2.8%)
| [12] | Arora MS, Kaushik R, Ahmad S, Kaushik RM. Profile of Acute Kidney Injury in Patients with Decompensated Cirrhosis at a Tertiary-Care Center in Uttarakhand, India. Dig Dis. 2020; 38(4): 335-343. |
[12]
. On the contrary, relatively higher proportion of advanced stages of AKI was depicted in studies by
Shetty S et al (stage 1: 15.4%%, stage 2: 26.8%%, stage 3: 57.7%%)
| [11] | Shetty S, Nagaraju SP, Shenoy S, Attur RP, Rangaswamy D, Rao IR et al. Acute kidney injury in patients with cirrhosis of liver: Clinical profile and predictors of outcome. Indian J Gastroenterol. 2018; 37(3): 248–254. |
[11]
and
Belcher J M et al (stage 1: 26%, stage 2: 24%, stage 3: 49%)
| [17] | Belcher JM, Garcia-Tsao G, Sanyal AJ, Bhogal H, Lim JK, Ansari N, et al; TRIBE-AKI Consortium. Association of AKI with mortality and complications in hospitalized patients with cirrhosis. Hepatology. 2013; 57(2): 753-62. |
[17]
.
Among patients with cirrhosis and AKI, most of the deceased patients belonged to stage 3 (66.7%) and stage 2 (29.2%) AKI, while only 1 patient (4.2%) had stage 1 AKI. Peak stage of AKI in cirrhosis was found to have significant association with mortality. 85% of patients with stage 2 and 3 AKI required ICU monitoring, depicting worse morbidity among advanced stages of AKI in cirrhosis. This data complies with studies by
Shetty S et al (stage 1: 15.8% vs stage 2: 27.3% vs stage 3: 60.6%)
| [11] | Shetty S, Nagaraju SP, Shenoy S, Attur RP, Rangaswamy D, Rao IR et al. Acute kidney injury in patients with cirrhosis of liver: Clinical profile and predictors of outcome. Indian J Gastroenterol. 2018; 37(3): 248–254. |
[11]
,
Kumar U et al (stage 2: 45.8% vs stage 3: 62.8%)
| [13] | Kumar U, Kumar R, Jha SK, Jha AK, Dayal VM, Kumar A. Short-term mortality in patients with cirrhosis of the liver and acute kidney injury: A prospective observational study. Indian J Gastroenterol. 2020; 39(5): 457-464. |
[13]
and
Scott R A et al (stage 1: 13.5% vs stage 2: 37.8% vs stage 3: 43.2%)
| [16] | Scott RA, Austin AS, Kolhe NV, McIntyre CW, Selby NM. Acute kidney injury is independently associated with death in patients with cirrhosis. Frontline Gastroenterol. 2013; 4(3): 191-197. |
[16]
.
5.4. Time of Onset of AKI in Patients with Cirrhosis
In our study population with cirrhosis, the majority had early onset AKI (at or within 24 hours of admission) rather than a delayed onset of AKI (onset after 24 hours of admission) (66.2% vs 33.8%). A relatively higher mortality rate was seen in cirrhotic patients with early onset AKI when compared to late onset AKI (46.9% vs 4%).
Kumar U et al also showed relatively higher proportion of cirrhotic patients with AKI at the time of admission than those with AKI during hospital course (67.2% vs 32.8%)
| [13] | Kumar U, Kumar R, Jha SK, Jha AK, Dayal VM, Kumar A. Short-term mortality in patients with cirrhosis of the liver and acute kidney injury: A prospective observational study. Indian J Gastroenterol. 2020; 39(5): 457-464. |
[13]
.
Hemodialysis: In our study, 13.5% of patients with cirrhosis and AKI, who all belonged to stage 3 AKI, underwent RRT and none of them survived.
Shetty S et al showed 17% patients with cirrhosis and AKI required hemodialysis
| [11] | Shetty S, Nagaraju SP, Shenoy S, Attur RP, Rangaswamy D, Rao IR et al. Acute kidney injury in patients with cirrhosis of liver: Clinical profile and predictors of outcome. Indian J Gastroenterol. 2018; 37(3): 248–254. |
[11]
, while in the study by
Arora MS et al, 21.1% of cirrhotic patients with AKI underwent RRT
| [12] | Arora MS, Kaushik R, Ahmad S, Kaushik RM. Profile of Acute Kidney Injury in Patients with Decompensated Cirrhosis at a Tertiary-Care Center in Uttarakhand, India. Dig Dis. 2020; 38(4): 335-343. |
[12]
.
5.5. Treatment Response in Patients with Cirrhosis and AKI
Among patients with cirrhosis and AKI, more than half made complete response (59.4%) when compared to partial responders (23%) and non-responders (17.6%). Mortality rate was significantly higher among non-responders (100%) and partial responders (58.8%) when compared to those who had complete response to treatment (2.3%).
Wong F et al also showed higher mortality rate among cirrhotic patients without renal recovery (80%) when compared to partial (40%) or complete recovery (15%) or patients without AKI (7%) (
p < 0.001)
| [18] | Wong F, O'Leary JG, Reddy KR, Patton H, Kamath PS, Fallon MB, et al. North American Consortium for Study of End-Stage Liver Disease. New consensus definition of acute kidney injury accurately predicts 30-day mortality in patients with cirrhosis and infection. Gastroenterology. 2013; 145(6): 1280-8. |
[18]
.
Treatment response significantly influenced the duration of hospital stay in patients with cirrhosis and AKI, as mean duration was higher in non-responder (12.8 ± 3.2 days), when compared to partial responders (10.1 ± 3.4 days) and complete responders (8.9 ± 2.5 days) to treatment. Mean duration of hospitalization significantly differed between non-responders and complete responders and thus, treatment response had significant impact on morbidity rate.
Our study is not without limitations. Firstly, the data provided in our study was based only on hospitalized patients with cirrhosis and hence, generalizing the data to the community may not be feasible. Secondly, renal biopsy to establish the definite cause of AKI could not be done due to inherent risk of bleeding in our cirrhotic patients. Thirdly, long term follow-up was not done in our study to assess long-term mortality rate and requirement for simultaneous liver-kidney transplantation. Finally, even though the need for liver transplantation (for patients fitting the criteria) was counselled to both patient and relatives, none of them could be taken up for transplantation primarily due to financial constraints.
6. Conclusion
The proportion of AKI in hospitalized patients with cirrhosis is significantly high (39.78%) in Northern Kerala. Patients with advanced cirrhosis, indicated by high CTP score, have a higher risk for AKI during hospitalization. Alcoholic liver disease, NAFLD and Hepatitis-B related cirrhosis comprised the majority of cirrhosis. Variceal bleeding and SBP are the most common risk factors for AKI in cirrhosis. Onset of AKI has a significant impact on the mortality and morbidity indices of patients with cirrhosis. Early stages of AKI are predominant among cirrhotic patients and mortality risk proportionately increases as the stage of AKI advances. Among the hospitalized cirrhotic patients with definite risk factors for AKI, close monitoring for early detection of the onset of AKI is essential for rapid institution of treatment.
Abbreviations
AKI | Acute Kidney Injury |
AKIN | Acute Kidney Injury Network |
ANOVA | Analysis of Variance |
AUROC | Area Under the Receiver Operating Characteristics |
CI | Confidence Interval |
CTP | Child-Turcotte-Pugh |
df | Degrees of Freedom |
HRS | Hepato-renal Syndrome |
ICA | International Club of Ascites |
ICU | Intensive Care Unit |
LRTI | Lower Respiratory Tract Infection |
LVP | Large Volume Paracentesis |
MELD | Model for End-stage Liver disease |
NAFLD | Non-alcoholic Fatty Liver Disease |
NSAID | Non-Steroidal Anti-inflammatory Drugs |
OR | Odds Ratio |
RRT | Renal Replacement Therapy |
SBP | Spontaneous Bacterial Peritonitis |
SD | Standard Deviation |
SPSS | Statistical Package for Social Sciences |
UTI | Urinary Tract Infection |
UGI | Upper Gastrointestinal |
Ethical Statement
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5). Informed consent was obtained from all patients for being included in the study.
Availability of Data and Material
The datasets used and analysed during the current study are available from corresponding author on reasonable request.
Author Contributions
Sandeep Menon: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review & editing
Sunil Kumar Kandiyil: Investigation, Supervision, Validation
Sithara Balagopal: Supervision
Kadavanoor Srijith: Supervision
Sandesh Kolassery: Supervision
Funding
Authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Ginès P, Schrier RW. Renal failure in cirrhosis. N Engl J Med. 2009; 361(13): 1279-90.
|
| [2] |
Wong F, Nadim MK, Kellum JA, Salerno F, Bellomo R, Gerbes A, et al. Working Party proposal for a revised classification system of renal dysfunction in patients with cirrhosis. Gut. 2011; 60(5): 702-9.
|
| [3] |
Wiesner R, Edwards E, Freeman R, Harper A, Kim R, Kamath P, et al; United Network for Organ Sharing Liver Disease Severity Score Committee. Model for end-stage liver disease (MELD) and allocation of donor livers. Gastroenterology. 2003; 124(1): 91-6.
|
| [4] |
Ginès P, Guevara M, Arroyo V, Rodés J. Hepatorenal syndrome. Lancet. 2003; 362(9398): 1819-27.
|
| [5] |
Angeli P, Gines P, Wong F, Bernardi M, Boyer TD, Gerbes A, et al; International Club of Ascites. Diagnosis and management of acute kidney injury in patients with cirrhosis: revised consensus recommendations of the International Club of Ascites. Gut. 2015; 64(4): 531-7.
|
| [6] |
Garcia-Martinez R, Noiret L, Sen S, Mookerjee R, Jalan R. Albumin infusion improves renal blood flow autoregulation in patients with acute decompensation of cirrhosis and acute kidney injury. Liver Int. 2015; 35(2): 335-43.
|
| [7] |
Wong F. Drug insight: the role of albumin in the management of chronic liver disease. Nat Clin Pract Gastroenterol Hepatol. 2007; 4(1): 43-51.
|
| [8] |
Gupta K, Bhurwal A, Law C, Ventre S, Minacapelli CD, Kabaria S, et al. Acute kidney injury and hepatorenal syndrome in cirrhosis. World J Gastroenterol. 2021; 27(26): 3984-4003.
|
| [9] |
Hampel H, Bynum GD, Zamora E, El-Serag HB. Risk factors for the development of renal dysfunction in hospitalized patients with cirrhosis. Am J Gastroenterol. 2001; 96(7): 2206-10.
|
| [10] |
Fagundes C, Barreto R, Guevara M, Garcia E, Solà E, Rodríguez E, et al. A modified acute kidney injury classification for diagnosis and risk stratification of impairment of kidney function in cirrhosis. J Hepatol. 2013; 59(3): 474-81.
|
| [11] |
Shetty S, Nagaraju SP, Shenoy S, Attur RP, Rangaswamy D, Rao IR et al. Acute kidney injury in patients with cirrhosis of liver: Clinical profile and predictors of outcome. Indian J Gastroenterol. 2018; 37(3): 248–254.
|
| [12] |
Arora MS, Kaushik R, Ahmad S, Kaushik RM. Profile of Acute Kidney Injury in Patients with Decompensated Cirrhosis at a Tertiary-Care Center in Uttarakhand, India. Dig Dis. 2020; 38(4): 335-343.
|
| [13] |
Kumar U, Kumar R, Jha SK, Jha AK, Dayal VM, Kumar A. Short-term mortality in patients with cirrhosis of the liver and acute kidney injury: A prospective observational study. Indian J Gastroenterol. 2020; 39(5): 457-464.
|
| [14] |
Tsien CD, Rabie R, Wong F. Acute kidney injury in decompensated cirrhosis. Gut. 2013; 62(1): 131-7.
|
| [15] |
Carvalho GC, Regis Cde A, Kalil JR, Cerqueira LA, Barbosa DS, Motta MP, et al. Causes of renal failure in patients with decompensated cirrhosis and its impact in hospital mortality. Ann Hepatol. 2012; 11(1): 90-5.
|
| [16] |
Scott RA, Austin AS, Kolhe NV, McIntyre CW, Selby NM. Acute kidney injury is independently associated with death in patients with cirrhosis. Frontline Gastroenterol. 2013; 4(3): 191-197.
|
| [17] |
Belcher JM, Garcia-Tsao G, Sanyal AJ, Bhogal H, Lim JK, Ansari N, et al; TRIBE-AKI Consortium. Association of AKI with mortality and complications in hospitalized patients with cirrhosis. Hepatology. 2013; 57(2): 753-62.
|
| [18] |
Wong F, O'Leary JG, Reddy KR, Patton H, Kamath PS, Fallon MB, et al. North American Consortium for Study of End-Stage Liver Disease. New consensus definition of acute kidney injury accurately predicts 30-day mortality in patients with cirrhosis and infection. Gastroenterology. 2013; 145(6): 1280-8.
|
Cite This Article
-
APA Style
Menon, S., Kandiyil, S. K., Balagopal, S., Sreejith, K., Kolassery, S. (2025). Acute Kidney Injury Among Hospitalised Patients with Cirrhosis – Burden and Risk Factors. International Journal of Gastroenterology, 9(1), 45-53. https://doi.org/10.11648/j.ijg.20250901.18
 Copy
|
Copy
|
 Download
Download
ACS Style
Menon, S.; Kandiyil, S. K.; Balagopal, S.; Sreejith, K.; Kolassery, S. Acute Kidney Injury Among Hospitalised Patients with Cirrhosis – Burden and Risk Factors. Int. J. Gastroenterol. 2025, 9(1), 45-53. doi: 10.11648/j.ijg.20250901.18
Copy
|
Download
AMA Style
Menon S, Kandiyil SK, Balagopal S, Sreejith K, Kolassery S. Acute Kidney Injury Among Hospitalised Patients with Cirrhosis – Burden and Risk Factors. Int J Gastroenterol. 2025;9(1):45-53. doi: 10.11648/j.ijg.20250901.18
Copy
|
Download
-
@article{10.11648/j.ijg.20250901.18,
author = {Sandeep Menon and Sunil Kumar Kandiyil and Sithara Balagopal and Kadavanoor Sreejith and Sandesh Kolassery},
title = {Acute Kidney Injury Among Hospitalised Patients with Cirrhosis – Burden and Risk Factors
},
journal = {International Journal of Gastroenterology},
volume = {9},
number = {1},
pages = {45-53},
doi = {10.11648/j.ijg.20250901.18},
url = {https://doi.org/10.11648/j.ijg.20250901.18},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijg.20250901.18},
abstract = {Background and Objectives: Acute Kidney Injury (AKI) in cirrhosis is a major determinant of morbidity and mortality. This study aims to assess the proportion, common predisposing factors and the mortality rate of hospitalised patients with AKI and cirrhosis. Methods: A single-center, longitudinal study was done in our setting including 186 patients with cirrhosis hospitalized to ward or ICU. AKI was diagnosed and staged as per ICA-AKI criteria. The proportion of AKI was calculated in percentage. Risk factors for AKI were recorded and their association was tested by chi-square test. Patient outcome (in terms of survived or deceased) was recorded and mortality rate was calculated in terms of percentage. Results: Proportion of AKI in hospitalized patients with cirrhosis was 39.7% (74/186). Alcoholic liver disease, NAFLD & hepatitis-B related cirrhosis comprised more than 90% of cirrhosis. Most patients with AKI had advanced stages of cirrhosis (CTP-A: 8, CTP-B: 18, CTP-C: 48). The common predisposing factors for AKI in cirrhotic patients were variceal bleeding (44.6%) and SBP (29.7%), while less common risk factors were infections like UTI (7%), LRTI (4%) and cellulitis (1.4%), along with large volume paracentesis (9.5%), recent over diuresis (8%), nephrotoxic drug intake (2.7%) and dehydration (1.4%). Most of the patients with cirrhosis who developed AKI had early stages of AKI. The mortality rate among hospitalized patients with cirrhosis and AKI was 32.4%. AKI was found to have a significant association with patient’s survival in cirrhosis. Conclusion: Burden of AKI, in terms of prevalence, morbidity as well as mortality among hospitalized patients with cirrhosis is significantly high in our region. Patients with definite predisposing factors require close monitoring for early detection of renal impairment.
},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Acute Kidney Injury Among Hospitalised Patients with Cirrhosis – Burden and Risk Factors
AU - Sandeep Menon
AU - Sunil Kumar Kandiyil
AU - Sithara Balagopal
AU - Kadavanoor Sreejith
AU - Sandesh Kolassery
Y1 - 2025/06/19
PY - 2025
N1 - https://doi.org/10.11648/j.ijg.20250901.18
DO - 10.11648/j.ijg.20250901.18
T2 - International Journal of Gastroenterology
JF - International Journal of Gastroenterology
JO - International Journal of Gastroenterology
SP - 45
EP - 53
PB - Science Publishing Group
SN - 2640-169X
UR - https://doi.org/10.11648/j.ijg.20250901.18
AB - Background and Objectives: Acute Kidney Injury (AKI) in cirrhosis is a major determinant of morbidity and mortality. This study aims to assess the proportion, common predisposing factors and the mortality rate of hospitalised patients with AKI and cirrhosis. Methods: A single-center, longitudinal study was done in our setting including 186 patients with cirrhosis hospitalized to ward or ICU. AKI was diagnosed and staged as per ICA-AKI criteria. The proportion of AKI was calculated in percentage. Risk factors for AKI were recorded and their association was tested by chi-square test. Patient outcome (in terms of survived or deceased) was recorded and mortality rate was calculated in terms of percentage. Results: Proportion of AKI in hospitalized patients with cirrhosis was 39.7% (74/186). Alcoholic liver disease, NAFLD & hepatitis-B related cirrhosis comprised more than 90% of cirrhosis. Most patients with AKI had advanced stages of cirrhosis (CTP-A: 8, CTP-B: 18, CTP-C: 48). The common predisposing factors for AKI in cirrhotic patients were variceal bleeding (44.6%) and SBP (29.7%), while less common risk factors were infections like UTI (7%), LRTI (4%) and cellulitis (1.4%), along with large volume paracentesis (9.5%), recent over diuresis (8%), nephrotoxic drug intake (2.7%) and dehydration (1.4%). Most of the patients with cirrhosis who developed AKI had early stages of AKI. The mortality rate among hospitalized patients with cirrhosis and AKI was 32.4%. AKI was found to have a significant association with patient’s survival in cirrhosis. Conclusion: Burden of AKI, in terms of prevalence, morbidity as well as mortality among hospitalized patients with cirrhosis is significantly high in our region. Patients with definite predisposing factors require close monitoring for early detection of renal impairment.
VL - 9
IS - 1
ER -
Copy
|
Download