This report presents a case treated with fire needle therapy combined with narrow-band ultraviolet B (NB-UVB) for chronic pityriasis lichenoides. The patient was a 44-year-old female who exhibited recurrent erythema, scaling, and pruritus on the limbs and trunk for a duration of five months. Dermatological examination revealed patchy bright red rashes on the chest with indistinct borders and no significant desquamation; scattered papules ranging from rice to soybean size, pale red to reddish-brown in color, were observed on the limbs, trunk, and buttocks, some of which were covered with fine, thin scales that shed easily. Additionally, patchy erythematous papules were noted on both palms, soles, and the dorsal aspects of the toes, accompanied by scattered vesicles and papules of similar size, some exhibiting minimal exudate and others covered with crusts. Nikolsky's sign was negative, and there was no thickening or deformation of the nails or toenails, nor were there palpable superficial lymph nodes. Dermatopathological findings revealed focal incomplete keratinization, neutrophilic exudate beneath the epidermis, mild epidermal hyperplasia, intercellular edema in the spinous layer, and liquefactive degeneration of the basal cells. A small number of lymphocytes were observed migrating into the epidermis, with lymphocyte-dominated inflammatory cell infiltration surrounding the blood vessels in the superficial to middle dermis, along with visible nuclear dust. The diagnosis was confirmed as chronic pityriasis lichenoides. Following one month of treatment with fire needle therapy in conjunction with NB-UVB irradiation, there was notable improvement in almost all clinical manifestations; the lesions on the chest completely resolved, and those on the dorsal feet became dry and convergent, with ongoing follow-up.
| Published in | International Journal of Medical Case Reports (Volume 3, Issue 3) |
| DOI | 10.11648/j.ijmcr.20240303.12 |
| Page(s) | 26-29 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Chronic Pityriasis Lichenoides, Fire Needle, Narrow-Band Ultraviolet B (NB-UVB)
NB-UVB | Narrow-band Ultraviolet b |
IgE | Immunoglobulin E |
PLC | Pityriasis Lichenoides Chronica |
PLEVA | Pityriasis Lichenoides et Varioliformis Acuta |
JAK | Janus Kinase |
TNF-α | Tumor Necrosis Factor-α |
IL-6 | Interleukin-6 |
IL-4 | Interleukin-4 |
| [1] | Juliusberg F. Ueber die Pityriasis lichenoides chronica: psoriasiform lichenoides Exanthem. Archiv für Dermatologie und Syphilis, 1899, 50(3): 359-374. |
| [2] | Giannetti A, Girolomoni G, Pincelli C, et al. Immunopathologic studies in pityriasis lichenoides. Archives of dermatological research, 1988, 280: S61-5. |
| [3] | Skinner R B, Levy A L. Rapid resolution of pityriasis lichenoides et varioliformis acuta with azithromycin. Journal of the American Academy of Dermatology, 2008, 58(3). |
| [4] | Franc M P, Barrut D, Moulin G. Pityriasis lichenoides (author's transl)//Annales de Dermatologie et de Venereologie. 1980, 107(10): 895-899. |
| [5] | Fink‐puches R, Chott A, Ardigó M, et al. The spectrum of cutaneous lymphomas in patients less than 20 years of age. Pediatric dermatology, 2004, 21(5): 525-533. |
| [6] | GANCHEVA R, POZHARASHKA J, KOUNDURDJIEV A, et al. A clinical case of pityriasis lichenoides chronica presenting with palpable purpura after streptococcal infection. Folia Medica, 2024, 66(3): 426-430. |
| [7] | Salah E M, Bedair N I, El‐rahim S K A, et al. Efficacy and safety of excimer light (308 nm) in the treatment of pityriasis lichenoides chronica. Photodermatology, Photoimmunology & Photomedicine, 2024, 40(3): e12964. |
| [8] | Obeng-Nyarko C N, DURANGO K P, JACKSON S, et al. Dupilumab for the treatment of Pityriasis Lichenoides Chronica: A Case Report. JAAD Case Reports, 2024. |
| [9] | Zhang Y, Liang Z, LI S, et al. Fire needle plus cupping for acute herpes zoster: study protocol for a randomized controlled trial. Trials, 2020, 21: 1-10. |
| [10] | Huang M, Tang L, Li X, et al. Clinical observation on therapeutic effect of filiform fire needle for vitiligo: a retrospective study. Dermatologic Therapy, 2020, 33(6): e14415. |
| [11] | Lee S, Kim S N. The effect of acupuncture on modulating inflammatory cytokines in rodent animal models of respiratory disease: A systematic review and meta-analysis. Frontiers in Immunology, 2022, 13: 878463. |
| [12] | Zhang Y, Chen C T, Huang S, et al. Efficacy observation of fire needle combined with narrow band ultraviolet-B (NB-UVB) for vitiligo. Zhongguo Zhen jiu= Chinese Acupuncture & Moxibustion, 2013, 33(2): 121-124. |
APA Style
Changchun, L., Jianping, S. (2024). A Case of Chronic Pityriasis Lichenoides Treated with Fire Needle Combined with Narrow-Band Ultraviolet B (NB-UVB) Irradiation. International Journal of Medical Case Reports, 3(3), 26-29. https://doi.org/10.11648/j.ijmcr.20240303.12
ACS Style
Changchun, L.; Jianping, S. A Case of Chronic Pityriasis Lichenoides Treated with Fire Needle Combined with Narrow-Band Ultraviolet B (NB-UVB) Irradiation. Int. J. Med. Case Rep. 2024, 3(3), 26-29. doi: 10.11648/j.ijmcr.20240303.12
AMA Style
Changchun L, Jianping S. A Case of Chronic Pityriasis Lichenoides Treated with Fire Needle Combined with Narrow-Band Ultraviolet B (NB-UVB) Irradiation. Int J Med Case Rep. 2024;3(3):26-29. doi: 10.11648/j.ijmcr.20240303.12
@article{10.11648/j.ijmcr.20240303.12,
author = {Lu Changchun and Shi Jianping},
title = {A Case of Chronic Pityriasis Lichenoides Treated with Fire Needle Combined with Narrow-Band Ultraviolet B (NB-UVB) Irradiation
},
journal = {International Journal of Medical Case Reports},
volume = {3},
number = {3},
pages = {26-29},
doi = {10.11648/j.ijmcr.20240303.12},
url = {https://doi.org/10.11648/j.ijmcr.20240303.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijmcr.20240303.12},
abstract = {This report presents a case treated with fire needle therapy combined with narrow-band ultraviolet B (NB-UVB) for chronic pityriasis lichenoides. The patient was a 44-year-old female who exhibited recurrent erythema, scaling, and pruritus on the limbs and trunk for a duration of five months. Dermatological examination revealed patchy bright red rashes on the chest with indistinct borders and no significant desquamation; scattered papules ranging from rice to soybean size, pale red to reddish-brown in color, were observed on the limbs, trunk, and buttocks, some of which were covered with fine, thin scales that shed easily. Additionally, patchy erythematous papules were noted on both palms, soles, and the dorsal aspects of the toes, accompanied by scattered vesicles and papules of similar size, some exhibiting minimal exudate and others covered with crusts. Nikolsky's sign was negative, and there was no thickening or deformation of the nails or toenails, nor were there palpable superficial lymph nodes. Dermatopathological findings revealed focal incomplete keratinization, neutrophilic exudate beneath the epidermis, mild epidermal hyperplasia, intercellular edema in the spinous layer, and liquefactive degeneration of the basal cells. A small number of lymphocytes were observed migrating into the epidermis, with lymphocyte-dominated inflammatory cell infiltration surrounding the blood vessels in the superficial to middle dermis, along with visible nuclear dust. The diagnosis was confirmed as chronic pityriasis lichenoides. Following one month of treatment with fire needle therapy in conjunction with NB-UVB irradiation, there was notable improvement in almost all clinical manifestations; the lesions on the chest completely resolved, and those on the dorsal feet became dry and convergent, with ongoing follow-up.
},
year = {2024}
}
TY - JOUR T1 - A Case of Chronic Pityriasis Lichenoides Treated with Fire Needle Combined with Narrow-Band Ultraviolet B (NB-UVB) Irradiation AU - Lu Changchun AU - Shi Jianping Y1 - 2024/12/25 PY - 2024 N1 - https://doi.org/10.11648/j.ijmcr.20240303.12 DO - 10.11648/j.ijmcr.20240303.12 T2 - International Journal of Medical Case Reports JF - International Journal of Medical Case Reports JO - International Journal of Medical Case Reports SP - 26 EP - 29 PB - Science Publishing Group SN - 2994-7049 UR - https://doi.org/10.11648/j.ijmcr.20240303.12 AB - This report presents a case treated with fire needle therapy combined with narrow-band ultraviolet B (NB-UVB) for chronic pityriasis lichenoides. The patient was a 44-year-old female who exhibited recurrent erythema, scaling, and pruritus on the limbs and trunk for a duration of five months. Dermatological examination revealed patchy bright red rashes on the chest with indistinct borders and no significant desquamation; scattered papules ranging from rice to soybean size, pale red to reddish-brown in color, were observed on the limbs, trunk, and buttocks, some of which were covered with fine, thin scales that shed easily. Additionally, patchy erythematous papules were noted on both palms, soles, and the dorsal aspects of the toes, accompanied by scattered vesicles and papules of similar size, some exhibiting minimal exudate and others covered with crusts. Nikolsky's sign was negative, and there was no thickening or deformation of the nails or toenails, nor were there palpable superficial lymph nodes. Dermatopathological findings revealed focal incomplete keratinization, neutrophilic exudate beneath the epidermis, mild epidermal hyperplasia, intercellular edema in the spinous layer, and liquefactive degeneration of the basal cells. A small number of lymphocytes were observed migrating into the epidermis, with lymphocyte-dominated inflammatory cell infiltration surrounding the blood vessels in the superficial to middle dermis, along with visible nuclear dust. The diagnosis was confirmed as chronic pityriasis lichenoides. Following one month of treatment with fire needle therapy in conjunction with NB-UVB irradiation, there was notable improvement in almost all clinical manifestations; the lesions on the chest completely resolved, and those on the dorsal feet became dry and convergent, with ongoing follow-up. VL - 3 IS - 3 ER -
Department of Dermatology, Guangzhou Red Cross Hospital, Jinan University, Guangzhou, China
Department of Dermatology, Guangzhou Red Cross Hospital, Jinan University, Guangzhou, China
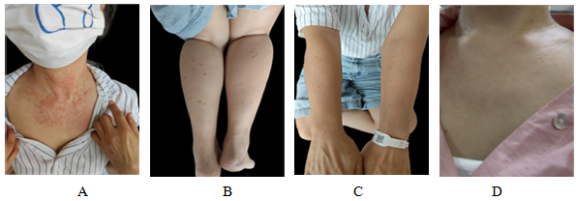
Figure 1. Clinical photos of the patient before and after treatment. A ~ C: Before treatment, on the chest, there are patchy erythemas with unclear boundaries and no obvious desquamation; there are scattered papules of rice to soybean size, pale red to reddish-brown in color, on both lower legs and the outer sides of the forearms, some covered with fine, thin scales that are easily shed; D: One month after treatment, there are scattered erythemas and papules on the chest, leaving scattered patchy brown pigmentation.
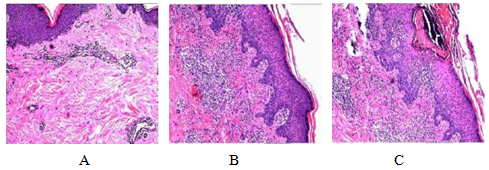
Figure 2. Histopathology: Focal parakeratosis, neutrophil exudate below, mild epidermal hyperplasia, intercellular edema in the spinous layer, liquefactive degeneration of basal cells in the basal layer, a small number of lymphocytes migrating into the epidermis, lymphocyte-dominated inflammatory cell infiltration around the blood vessels in the superficial to middle dermis, and visible nuclear dust.
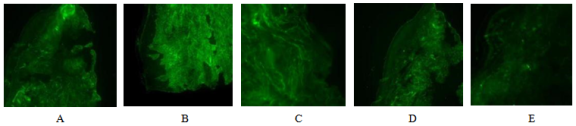
Figure 3. Immunofluorescence results(A-E): IgG, IgA, IgM, C3 and C4 are all negative.
Information

