Background: Huge craniofacial tumors represent a surgical challenge not only for high risk of intraoperative damage of the brain and sense organs of the face, but also for esthetical issues which may occur postoperatively. This surgery is riskier when these processes are represented by massive compact bone such as osteomas. Case presentation: A young patient with huge disfiguring osteoma of anterior skull base extended to sphenoidal, frontal, maxillary sinuses as well as in orbits benefit for a complete removal with craniofacial reconstruction through a surgical teamwork including neurosurgeon, maxillofacial surgeon and ophthalmologist; with an overt satisfactory cosmetic result. Preoperative planning is reported as well as the intraoperative procedure and the postoperative reconstruction and follow up. Conclusion: Craniofacial osteoma represents a surgical and cometic challenge for their resection. This resection is tailored through sophisticated devices such as preoperative 3D (3 dimension) printed model, intraoperative neuronavigation, and the use on custom-made bone. In place where this reported patient is managed, these tools are unavailable. Thus, priority should be given to teamwork with accurate preoperative planning and manually confectioned cranioplasty. Endoscopic approach for these processes gained more and more indication in the resection of these craniofacial and skull base osteomas. Since this device require a learning curve, laboratory training for is proper using as well as in microneurosurgery techniques is highly recommended. A hope is encountered though the humanitarian implication of some organization and universities.
| Published in | International Journal of Neurosurgery (Volume 8, Issue 1) |
| DOI | 10.11648/j.ijn.20240801.13 |
| Page(s) | 16-21 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Osteoma, Craniofacial Sinuses, Skull Base, Orbit, Cranioplasty, Endoscopy, Microneurosurgery Laboratory
3D | 3 Dimensions |
CT Scan | Computed Tomography Scan |
| [1] | Sendul SY, Mavi Yildiz A, Yildiz AA. Giant osteomas: Clinical results and surgical approach from ophthalmic point of view. Eur J Ophthalmol. 2021; 31(2): 766-773. |
| [2] | Torun MT, Turan F, Tuncel U. Giant ethmoid osteoma originated from the lamina papyracea. Med Arh. 2014; 68(3): 209-211. |
| [3] | Wang TH, Ma H, Huang LY, Hung YC, Wang TH, Yu WC, Chiu FY, Wang SJ, Chen WM. Printing a patient-specific instrument guide for skull osteoma management. J Chin Med Assoc. 2020; 83(10): 918-922. |
| [4] | Haddad FS, Haddad GF, Zaatari G. Cranial osteomas: their classification and management. Report on a giant osteoma and review of the literature. Surg Neurol. 1997; 48(2): 143-147. |
| [5] | Humeniuk-Arasiewicz M, Stryjewska-Makuch G, Janik MA, Kolebacz B. Giant fronto-ethmoidal osteoma - selection of an optimal surgical procedure. Braz J Otorhinolaryngol. 2018; 84(2): 232-239. |
| [6] | Mugliston T. A. H, Stafford N. A cranio-facial approach to large osteomas of the fronto-ethmoidal region, J. Laryngol. Otol. 1985; 99 (10): 979–983. |
| [7] | Shady J. A, Bland L. I, Kazee A. M, Pilcher W. H. Osteoma of the Fronto-ethmoidal Sinus with Secondary Brain Abscess and Intracranial Mucocele: Case Report. Neurosurgery. 1994 34 (5) 920–923. |
| [8] | Elwatidy S, Alkhathlan M, Alhumsi T, Kattan A, Al-Faky Y, Alessa, M. Strategy for surgical excision and primary reconstruction of giant frontal sinus osteoma. Interdisciplinary Neurosurgery: Advanced Techniques and Case Management. 2021; 23. Article 100905. |
| [9] | Olumide AA, Fajemisin AA, Adeloye A: Osteoma of the ethmofrontal sinus. Case report. J Neurosurg. 1975; 42: 343-345. |
| [10] | Lunardi P, Missori P, Di Lorenzo N, Fortuna A. Giant intracranial mucocele secondary to osteoma of the frontal sinuses: Report of two cases and review of the literature. Surgical Neurology. 1993; 39(1): 46–48. |
| [11] | Rappaport J. M, Attia E. L. Pneumocephalus in frontal sinus osteoma: a case report. J Otolaryngol. 1994; 23: 430–436. |
| [12] | Badakere A and Patil-Chhablani P. Orbital apex syndrome: a review. Eye Brain. 2019; 11: 63–72. |
| [13] | Cheng KJ, Wang SQ, Lin L. Giant osteomas of the ethmoid and frontal sinuses: clinical characteristics and review of the literature. Oncol Lett. 2013; 5: 1724-1730. |
| [14] | Blanco Dominguez I, Oteiza Alvarez AV, Martinez Gonzalez LM, Moreno Garcia-Rubio B, Franco Iglesias G, Riba Garcia J. Fronto-ethmoidal osteoma with orbital extension. A case report. Arch Soc Esp Oftalmol. 2016; 91: 349-352. |
| [15] | Nagashima H, Aihara H, Tashiro T, Kohmura E. Brain abscess associated with ethmoidal sinus osteoma: a case report. INAT. 2014; 1: 97-100. |
| [16] | Savastano M, Guarda-Nardini L, Marioni G, Staffieri A. The bicoronal approach for the treatment of a large frontal sinus osteoma. A technical note. Am J Otolaryngol. 2007; 28: 427-429. |
| [17] | Alotaibi N, Hanss J, Benoudiba F, Bobin S, Racy E. Endoscopic removal of large orbito-ethmoidal osteoma in pediatric patient: case report. Int J Surg Case Rep. 2013; 4: 1067-1070. |
| [18] | Oles K, Strek P, Wiatr M, Szaleniec J. Endoscopic treatment of giant skull base osteomas. Otolaryngol Pol. 2011; 65: 410-413. |
| [19] | Lee DH, Jung SH, Yoon TM, Lee JK, Joo YE, Lim SC. Characteristics of paranasal sinus osteoma and treatment outcomes. Acta Otolaryngol. 2015; 135: 602-607. |
| [20] | Müslüman AM, Oba E, Yilmaz A, Kabukcuoglu F, Uysal E. Giant osteoid osteoma of the ethmoid bone with unusual large nidus. J Neurosci Rural Pract. 2012; 3: 383-385. |
| [21] |
Abou Al-Shaar H, El Arjani T, Timms MS, Al-Otaibi F. Giant orbitoethmoidal osteoma: when an open surgical approach is required. Case Rep Otolaryngol. 2015: 872038.
https://doi.org/10.1155/2015/872038 Epub 2015 Mar 23 |
| [22] | Keles A, Cancela AA, Moussalem CK, Kessely YC, Malazonia Z, Shah JM, Gurbuz MS, Gasimov T, Adekanmbi A, Bari MS, Dumot C, Oriola GG, Golidtum JPU, Bin Mohd Nor MA, Omar AH, Ozaydin B, Patel NJ, Dempsey RJ, Baskaya MK. A Novel Approach for Free, Affordable, and Sustainable Microsurgery Laboratory Training for Low- and Middle-Income Countries: University of Wisconsin-Madison Microneurosurgery Laboratory Experience. Neurosurgery. 2024 Jan 30. |
| [23] | Dao I, Kièmtoré A, Ouattara O, Bako F, Traoré J, Biogo J, Yameogo SP, Sanou A, Kienou E, Comboigo LJ, Tossou A, Thiombiano A, Taoko L, Lankoande H, Nassoum E, Ouédraogo N, Adéniran SF, Somda A, Zabsonré DS, Kabré A. Periventricular and Intraventricular Tumors in a Low-Income Country: Hard Learning Curve and Outcome of a Young Neurosurgeon from Burkina Faso. Int J Neurosurg. 2024; 8(1): 1-10. |
APA Style
Dao, I., Traoré, I., Kohoun, M., Somda, A., Sow, S., et al. (2024). 400 Gramme on Skull Base and Face: Complete Removal and Reconstruction. International Journal of Neurosurgery, 8(1), 16-21. https://doi.org/10.11648/j.ijn.20240801.13
ACS Style
Dao, I.; Traoré, I.; Kohoun, M.; Somda, A.; Sow, S., et al. 400 Gramme on Skull Base and Face: Complete Removal and Reconstruction. Int. J. Neurosurg. 2024, 8(1), 16-21. doi: 10.11648/j.ijn.20240801.13
AMA Style
Dao I, Traoré I, Kohoun M, Somda A, Sow S, et al. 400 Gramme on Skull Base and Face: Complete Removal and Reconstruction. Int J Neurosurg. 2024;8(1):16-21. doi: 10.11648/j.ijn.20240801.13
@article{10.11648/j.ijn.20240801.13,
author = {Ibrahim Dao and Ibrahima Traoré and Michel Kohoun and Astride Somda and Salah Sow and Nasser Doukouré and Narcisse Ouedraogo and Ousmane Ouattara and Frédéric Bako and Abdoulaye Sanou and Elie Dibloni Nassoum and Arsène Tossou and Rasmané Beogo and Patrick Wendpouiré Hamed Dakouré},
title = {400 Gramme on Skull Base and Face: Complete Removal and Reconstruction
},
journal = {International Journal of Neurosurgery},
volume = {8},
number = {1},
pages = {16-21},
doi = {10.11648/j.ijn.20240801.13},
url = {https://doi.org/10.11648/j.ijn.20240801.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijn.20240801.13},
abstract = {Background: Huge craniofacial tumors represent a surgical challenge not only for high risk of intraoperative damage of the brain and sense organs of the face, but also for esthetical issues which may occur postoperatively. This surgery is riskier when these processes are represented by massive compact bone such as osteomas. Case presentation: A young patient with huge disfiguring osteoma of anterior skull base extended to sphenoidal, frontal, maxillary sinuses as well as in orbits benefit for a complete removal with craniofacial reconstruction through a surgical teamwork including neurosurgeon, maxillofacial surgeon and ophthalmologist; with an overt satisfactory cosmetic result. Preoperative planning is reported as well as the intraoperative procedure and the postoperative reconstruction and follow up. Conclusion: Craniofacial osteoma represents a surgical and cometic challenge for their resection. This resection is tailored through sophisticated devices such as preoperative 3D (3 dimension) printed model, intraoperative neuronavigation, and the use on custom-made bone. In place where this reported patient is managed, these tools are unavailable. Thus, priority should be given to teamwork with accurate preoperative planning and manually confectioned cranioplasty. Endoscopic approach for these processes gained more and more indication in the resection of these craniofacial and skull base osteomas. Since this device require a learning curve, laboratory training for is proper using as well as in microneurosurgery techniques is highly recommended. A hope is encountered though the humanitarian implication of some organization and universities.
},
year = {2024}
}
TY - JOUR T1 - 400 Gramme on Skull Base and Face: Complete Removal and Reconstruction AU - Ibrahim Dao AU - Ibrahima Traoré AU - Michel Kohoun AU - Astride Somda AU - Salah Sow AU - Nasser Doukouré AU - Narcisse Ouedraogo AU - Ousmane Ouattara AU - Frédéric Bako AU - Abdoulaye Sanou AU - Elie Dibloni Nassoum AU - Arsène Tossou AU - Rasmané Beogo AU - Patrick Wendpouiré Hamed Dakouré Y1 - 2024/05/24 PY - 2024 N1 - https://doi.org/10.11648/j.ijn.20240801.13 DO - 10.11648/j.ijn.20240801.13 T2 - International Journal of Neurosurgery JF - International Journal of Neurosurgery JO - International Journal of Neurosurgery SP - 16 EP - 21 PB - Science Publishing Group SN - 2640-1959 UR - https://doi.org/10.11648/j.ijn.20240801.13 AB - Background: Huge craniofacial tumors represent a surgical challenge not only for high risk of intraoperative damage of the brain and sense organs of the face, but also for esthetical issues which may occur postoperatively. This surgery is riskier when these processes are represented by massive compact bone such as osteomas. Case presentation: A young patient with huge disfiguring osteoma of anterior skull base extended to sphenoidal, frontal, maxillary sinuses as well as in orbits benefit for a complete removal with craniofacial reconstruction through a surgical teamwork including neurosurgeon, maxillofacial surgeon and ophthalmologist; with an overt satisfactory cosmetic result. Preoperative planning is reported as well as the intraoperative procedure and the postoperative reconstruction and follow up. Conclusion: Craniofacial osteoma represents a surgical and cometic challenge for their resection. This resection is tailored through sophisticated devices such as preoperative 3D (3 dimension) printed model, intraoperative neuronavigation, and the use on custom-made bone. In place where this reported patient is managed, these tools are unavailable. Thus, priority should be given to teamwork with accurate preoperative planning and manually confectioned cranioplasty. Endoscopic approach for these processes gained more and more indication in the resection of these craniofacial and skull base osteomas. Since this device require a learning curve, laboratory training for is proper using as well as in microneurosurgery techniques is highly recommended. A hope is encountered though the humanitarian implication of some organization and universities. VL - 8 IS - 1 ER -
Department of Orthopedic Surgery, University Hospital Souro Sanou, Bobo Dioulasso, Burkina Faso; Higher Institute of Health Sciences, Nazi Boni University, Bobo Dioulasso, Burkina Faso; Department Surgery, Military Hospital Colonel Major Tanguet Ouattara, Bobo Dioulasso, Burkina Faso
Department of Neurosurgery, University Hospital Yalgado Ouedraogo, Joseph Ki-Zerbo University, Ouagadougou, Burkina Faso
Department of Radiology and Medical Imaging, University Hospital Yalgado Ouedraogo, Joseph Ki-Zerbo University, Ouagadougou, Burkina Faso
Department of Orthopedic Surgery, University Hospital Souro Sanou, Bobo Dioulasso, Burkina Faso
Department of Orthopedic Surgery, University Hospital Souro Sanou, Bobo Dioulasso, Burkina Faso
Department of Orthopedic Surgery, University Hospital Souro Sanou, Bobo Dioulasso, Burkina Faso
Department of Neurosurgery, University Hospital Yalgado Ouedraogo, Joseph Ki-Zerbo University, Ouagadougou, Burkina Faso; Department of Neurosurgery, Military Hospital Capitaine Halassane Coulibaly, Ouagadougou, Burkina Faso
Department of Neurosurgery, University Hospital Yalgado Ouedraogo, Joseph Ki-Zerbo University, Ouagadougou, Burkina Faso; Department of Neurosurgery, Military Hospital Capitaine Halassane Coulibaly, Ouagadougou, Burkina Faso
Department of Neurosurgery, University Hospital Yalgado Ouedraogo, Joseph Ki-Zerbo University, Ouagadougou, Burkina Faso; Department of Neurosurgery, Military Hospital Capitaine Halassane Coulibaly, Ouagadougou, Burkina Faso

Figure 1. Craniofacial CT scan showing a multilobulated bony mass of the antérior skull base, extended to the sinuses, orbit and nasal cavities.
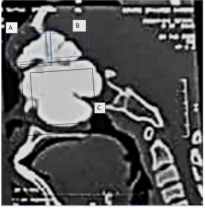
Figure 2. Surgical planning: Anterior room of the first floor (A), posterior room of the first floor (B) and the ground floor (C).
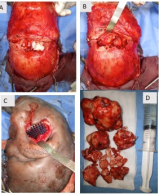
Figure 3. Intraoperative images showing mucocele (A), osteoma in frontal sinuses (B), reconstruction of the floor of orbit (C) and osteoma resection at the end of the surgery (D).
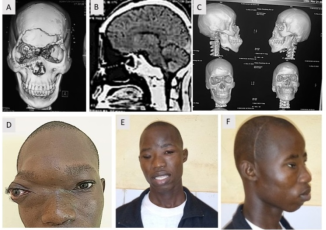
Figure 4. Post operative CT Scan showing a complet removal of the osteoma (A, B) with cranioplasty (C). preoperative picture (D) compatively to post operative shows the cosmetic result.
Information

