Low birth weight (LBW), defined by the World Health Organization as a birth weight of less than 2.5 kilograms, is a major public health concern with significant implications for neonatal morbidity, mortality, and long-term health outcomes. LBW prevalence is particularly high in developing countries, contributing to substantial healthcare challenges and socio-economic burdens. This study examines the determinants of LBW in Nigeria, focusing on socio-demographic, economic, and health-related factors. This cross-sectional study utilizes data from the 2018 Nigeria Demographic and Health Survey (NDHS). A stratified two-stage cluster sampling method was employed, and data were collected through structured interviews. The analysis included socio-demographic characteristics, economic status, health factors, and birth weights, which were classified into LBW and normal birth weight categories. Ethical approval was obtained, and informed consent ensured participant confidentiality. The analysis revealed significant associations between LBW and several factors. Higher maternal education levels were linked to lower odds of LBW. Religious affiliation also impacted LBW, with Muslim mothers having a lower likelihood of LBW compared to Christian mothers. Ethnicity influenced LBW outcomes, with Igbo mothers showing higher odds of LBW compared to Yoruba mothers. Economic stability and urban residency were associated with reduced LBW risk. Health factors such as maternal BMI and frequent antenatal visits were protective against LBW. Geographic disparities indicated higher risks in northern Nigeria. The study underscores the multifactorial nature of LBW, highlighting the importance of maternal education, socio-economic support, and healthcare access. Tailored interventions addressing ethnic and religious contexts, along with region-specific strategies, are essential. The Bayesian STAR model's superior performance suggests that spatial and non-parametric considerations provide deeper insights into LBW risk factors. Comprehensive, multifaceted strategies and policies are needed to address the determinants of LBW, focusing on vulnerable populations and regional disparities.
| Published in | Journal of Family Medicine and Health Care (Volume 10, Issue 3) |
| DOI | 10.11648/j.jfmhc.20241003.11 |
| Page(s) | 40-50 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Low Birth Weight (LBW), Socio-Demographic Factors, Economic Status, Maternal Education, Bayesian STAR Model
Variables | Levels | Posterior Mean | Odds Ratio | Posterior SD | Lower C. I. | Upper C. I. |
|---|---|---|---|---|---|---|
Intercept | -1.124 | 0.3862 | 0.1524 | 0.6843 | ||
Level of Education | No education (RC) | 1 | ||||
Primary | -0.1514 | 0.86 | 0.2969 | 0.4778 | 1.5773 | |
Secondary | -0.5136 | 0.60 | 0.269 | 0.3612 | 1.0162 | |
Higher | -0.6228 | 0.54 | 0.2808 | 0.3146 | 0.9249 | |
Religion | Christianity (RC) | 1 | ||||
Islam | -0.0474 | 0.95 | 0.2037 | 0.9481 | 2.1140 | |
Others | 2.5698 | 13.06 | 1.4614 | 0.9850 | 339.75 | |
Ethnicity | Yoruba (RC) | 1 | ||||
Hausa | -0.1758 | 0.84 | 0.3731 | 0.3997 | 1.7600 | |
Igbo | 0.1273 | 1.136 | 0.2929 | 0.6311 | 2.0381 | |
Others | -0.156 | 0.86 | 0.2498 | 0.5332 | 1.3910 | |
Gender of Child | Male (RC) | 1 | ||||
Female | 0.1259 | 1.14 | 0.1403 | 0.8626 | 1.4761 | |
Birth Interval | 1st Birth (RC) | 1 | ||||
<36 Months | -0.2022 | 0.82 | 0.0001 | 0.8168 | 0.8187 | |
36+ Months | -0.1666 | 0.85 | 0.0002 | 0.8454 | 0.8471 | |
Employment Status | Not Working (RC) | 1 | ||||
Working | -0.0169 | 0.98 | 0.002 | 0.9822 | 0.9840 | |
Wealth Index | Poorest (RC) | 1 | ||||
Poorer | 0.3312 | 1.39 | 0.0016 | 1.3925 | 1.4002 | |
Middle | 0.1228 | 1.13 | 0.0001 | 1.1299 | 1.1308 | |
Richer | -0.3438 | 0.71 | 0.3897 | 0.3160 | 1.4723 | |
Richest | -0.3611 | 0.70 | 0.3999 | 0.3421 | 1.7112 | |
Maternal BMI | Under-weight (RC) | 1 | ||||
Normal weight | -0.4175 | 0.66 | 0.0001 | 0.6578 | 1.6019 | |
Obesity | 0.4135 | 1.51 | 0.3264 | 0.7975 | 2.8207 | |
No of Ante-natal visits | No Visit (RC) | 1 | ||||
1 - 3 Visits | -0.2367 | 0.79 | 0.3145 | 0.4142 | 1.4299 | |
4 - 7 Visits | -0.2539 | 0.78 | 0.1659 | 0.5626 | 1.7784 | |
Above 7 Visits | -0.1403 | 0.87 | 0.1992 | 0.5778 | 1.2799 | |
Presence of Fever | No (RC) | 1 | ||||
Yes | 0.2308 | 1.26 | 0.1759 | 0.8887 | 1.7818 | |
Residential Type | Urban (RC) | 1 | ||||
Rural | 0.2286 | 1.26 | 0.0011 | 1.2481 | 1.2572 | |
Geographical Zone | North Central (RC) | 1 | ||||
North East | -0.2626 | 0.77 | 0.33 | 0.4070 | 1.4174 | |
North West | 0.0721 | 1.08 | 0.3797 | 0.4933 | 2.3030 | |
South East | -0.9071 | 0.40 | 0.2981 | 0.2313 | 0.7344 | |
South South | -0.2238 | 0.80 | 0.2495 | 0.5030 | 1.2755 | |
South West | -0.0916 | 0.91 | 0.2375 | 0.5830 | 1.4566 | |
Drinking Water | Unimproved (RC) | 1 | ||||
Improved | -0.186 | 0.8303 | 0.012 | 0.61348 | 1.12547 | |
Type of Cooking Fuel | Electricity (RC) | 1 | ||||
Gas | -0.0135 | 0.9866 | 0.0111 | 0.51234 | 1.04142 | |
Smoking | 0.1231 | 1.1310 | 0.0005 | 0.78121 | 1.56911 | |
Type of Toilet Facilities | Unimproved (RC) | 1 | ||||
Improved | -0.1181 | 0.8886 | 0.022 | 0.53526 | 1.62466 |
Variable | Posterior Mean | Posterior SD | 2.50% | 97.50% | Min | Max |
|---|---|---|---|---|---|---|
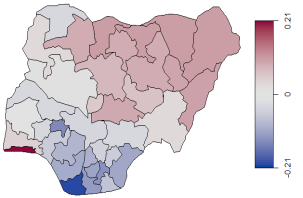
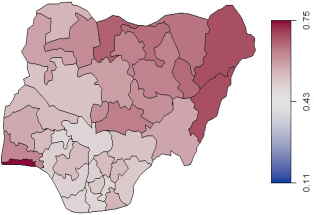
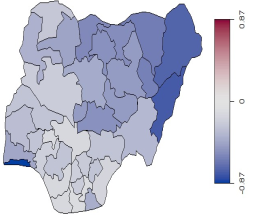
Geographical location | 0.7214 | 0.6203 | 0.0197 | 2.2897 | 0.0027 | 4.1629 |
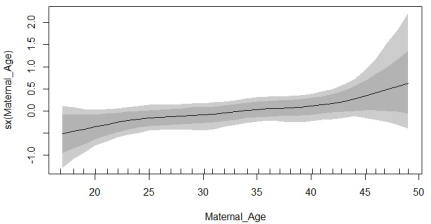
Maternal Age | 0.0087 | 0.0226 | 0.0005 | 0.0433 | 0.0003 | 0.4743 |
Variables | Category | Exp (B) | Lower C. I. | Upper C. I. | Sig. |
|---|---|---|---|---|---|
Intercept | |||||
Level of Education | No education (RC) | 1 | |||
Primary | 2.12 | 1.111 | 4.028 | 0.023 | |
Secondary | 1.78 | 1.055 | 2.995 | 0.031 | |
Higher | 1.22 | 0.834 | 1.773 | 0.309 | |
Religion | Christianity (RC) | 1 | |||
Islam | 0.072 | 0.005 | 0.981 | 0.048 | |
Others | 0.104 | 0.007 | 1.46 | 0.093 | |
Ethnicity | Yoruba (RC) | 1 | |||
Hausa | 1.388 | 0.758 | 2.54 | 0.288 | |
Igbo | 0.8 | 0.363 | 1.763 | 0.58 | |
Others | 1.461 | 0.782 | 2.729 | 0.235 | |
Gender of Child | Male (RC) | 1 | |||
Female | 0.915 | 0.692 | 1.208 | 0.53 | |
Birth Interval | 1st Birth (RC) | 1 | |||
<36 Months | 1.227 | 0.807 | 1.866 | 0.339 | |
36+ Months | 0.864 | 0.607 | 1.229 | 0.417 | |
Residential Type | Urban (RC) | 1 | |||
Rural | 1.963 | 0.429 | 8.995 | 0.385 | |
Employment Status | Not Working (RC) | 1 | |||
Working | 1.07 | 0.755 | 1.517 | 0.703 | |
Wealth Index | Poorest (RC) | 1 | |||
Poorer | 0.949 | 0.399 | 2.261 | 0.906 | |
Middle | 1.386 | 0.755 | 2.544 | 0.292 | |
Richer | 0.766 | 0.473 | 1.242 | 0.28 | |
Richest | 1.118 | 0.774 | 1.614 | 0.553 | |
Maternal BMI | Under weight (RC) (< 18.5) | 1 | |||
Normal weight (18.5-24.9) | 1.479 | 0.758 | 2.886 | 0.251 | |
Obesity (≥25) | 1.675 | 1.218 | 2.303 | 0.001 | |
No of Ante-natal visits | No Visit (RC) | 1 | |||
1 - 3 Visits | 1.201 | 0.812 | 1.776 | 0.359 | |
4 - 7 Visits | 0.965 | 0.479 | 1.944 | 0.921 | |
Above 7 Visits | 0.663 | 0.298 | 1.475 | 0.314 | |
Malaria in pregnancy | No (RC) | 1 | |||
Yes | 0.99 | 0.692 | 1.418 | 0.958 | |
Geographical Zone | North Central (RC) | 1 | |||
North East | 1.102 | 0.612 | 1.987 | 0.746 | |
North West | 1.135 | 0.296 | 4.356 | 0.853 | |
South East | 0.952 | 0.348 | 2.603 | 0.924 | |
South South | 0.463 | 0.232 | 0.924 | 0.029 | |
South West | 1.036 | 0.522 | 2.055 | 0.92 |
Models | ||
|---|---|---|
Statistitcs | Logistic | Bayesian STAR |
-2 log likelihood | 1391.069 | 917.671 |
Cox and snell R2 | 0.065 | 0.093 |
P-value of Models | 0.000 | 0.000 |
Chi-Square | 135.085 | 140.055 |
LBN | Low Birth Weight |
MCMC | Markov Chain Monte Carlo |
WHO | World Health Organisation |
LMICs | Low and Middle-Income Countries |
GLM | Generalized Linea Model |
GAM | Generalized Additive Model |
| [1] | Ngwira, A. (2019). Spatial quantile regression with application to high and low child birth weight in Malawi. 1–11. |
| [2] | Mahumud, R. A., Sultana, M., & Sarker, A. R. (2017a). Distribution and determinants of low birth weight in developing countries. Journal of Preventive Medicine and Public Health, 50(1), 18–28. |
| [3] | Ngwira, A., & Stanley, C. C. (2015). Determinants of Low Birth Weight in Malawi: Bayesian Geo-Additive Modelling. 1–14. |
| [4] | Muchemi, O. M., Echoka, E., & Makokha, A. (2015). Factors associated with low birth weight among neonates born at Olkalou district hospital, central region, Kenya. Pan African Medical Journal, 20, 1–11. |
| [5] | Ge, H., Liu, W., Li, H., Zhang, M., Zhang, M., Liu, C., & Qiao, Y. (2021). The association of vitamin D and vitamin E levels at birth with bronchopulmonary dysplasia in preterm infants. Pediatric Pulmonology. |
| [6] | Blanc, A. K., & Wardlaw, T. (2005). Monitoring low birth weight: An evaluation of international estimates and an updated estimation procedure. Bulletin of the World Health Organization, 83(3), 178–185. |
| [7] | Cutland, C. L., Lackritz, E. M., Mallett-Moore, T., Bardají, A., Chandrasekaran, R., Lahariya, C., Nisar, M. I., Tapia, M. D., Pathirana, J., Kochhar, S., & Muñoz, F. M. (2017). Low birth weight: Case definition & guidelines for data collection, analysis, and presentation of maternal immunization safety data. Vaccine, 35(48), 6492–6500. |
| [8] | Endalamaw, A., Engeda, E. H., Ekubagewargies, D. T., Belay, G. M., & Tefera, M. A. (2018). Low birth weight and its associated factors in Ethiopia: A systematic review and meta-analysis. Italian Journal of Pediatrics, 44(1). |
| [9] | Dahlui, M., Azahar, N., Oche, O. M., & Aziz, N. A. (2017). Risk factors for low birth weight in Nigeria: Evidence from the 2013 Nigeria Demographic and Health Survey. Global Health Action, 9, 28822. |
| [10] | Gathimba, N. W., Wanjoya, A., Kiplagat, G. K., Mbugua, L., & Kibiwott, K. (2017). Modeling Maternal Risk Factors Affecting Low Birth Weight Among Infants in Kenya. American Journal of Theoretical and Applied Statistics, 6(1), 22–31. |
| [11] | Manyeh, A. K., Kukula, V., Odonkor, G., Ekey, R. A., Adjei, A., Narh-bana, S., Akpakli, D. E., & Gyapong, M. (2016). Socioeconomic and demographic determinants of birth weight in southern rural Ghana: Evidence from Dodowa Health and Demographic Surveillance System. BMC Pregnancy and Childbirth, 1–9. |
| [12] | Desai, S., & Alva, S. (1998). Maternal education and child health: Is there a strong causal relationship?. Demography, 35(1), 71-81. |
| [13] | Kana, M. A., Doctor, H. V., Peleteiro, B., et al. (2015). Maternal and child health interventions in Nigeria: A systematic review of published studies from 1990 to 2014. BMC Public Health, 15, 334. |
| [14] | Matsas, A., Panopoulou, P., Antoniou, N., Bargiota, A., Gryparis, A., Vrachnis, N., Mastorakos, G., Kalantaridou, S. N., Panoskaltsis, T., Vlahos, N. F., & Valsamakis, G. (2023). Chronic stress in pregnancy is associated with low birth weight: A meta-analysis. Journal of Clinical Medicine, 12(24), 7686. |
| [15] | Agyemang, C., van Oeffelen, A. A., Norredam, M., & Zarrinkoub, R. (2009). The effect of neighbourhood income and deprivation on pregnancy outcomes in Amsterdam, The Netherlands. Journal of Epidemiology and Community Health, 63(9), 755-760. |
| [16] | Thapa, P., Poudyal, A., Poudel, R., Upadhyaya, D. P., Timalsina, A., Bhandari, R., Baral, J., Bhandari, R., Joshi, P. C., Thapa, P., & Adhikari, N. (2022). Prevalence of low birth weight and its associated factors: Hospital based cross-sectional study in Nepal. PLOS Global Public Health, 2(11), e0001220. |
| [17] | K, C. A., Basel, P. L., & Singh, S. (2020). Low birth weight and its associated risk factors: Health facility-based case-control study. PLoS One, 15(6), e0234907. |
| [18] | Dagdeviren, H., Donoghue, M., & Promberger, M. (2015). Resilience, Hardship and Social Conditions. Journal of Social Policy, 45, |
| [19] | Goldenberg, R. L., Culhane, J. F., Iams, J. D., & Romero, R. (2008). Epidemiology and causes of preterm birth. Lancet, 371(9606), 75-84. |
| [20] | Kramer, M. S., & Kakuma, R. (2003). Energy and protein intake in pregnancy. Cochrane Database of Systematic Reviews, 4, CD000032. |
| [21] |
Lincetto, O., Mothebesoane-Anoh, S., Gomez, P., & Munjanja, S. (2012). Opportunities for Africa’s Newborns. Antenatal Care.
https://www.who.int/entity/pmnch/media/publications/aonsectionIII_2.pdf |
| [22] | Gharoro, E. P., & Igbafe, A. A. (2002). Maternal Age First Birth and Obstetric Outcome. Nigerian Journal of Clinical Practice, 5, 20-24. |
| [23] | Cleary-Goldman, J., Malone, F. D., Vidaver, J., Ball, R. H., Nyberg, D. A., Comstock, C. H.,... & D’Alton, M. E. (2005). Impact of maternal age on obstetric outcome. Obstetrics & Gynecology, 105(5), 983-990. |
| [24] | Gelfand, A. E., Diggle, P. J., Fuentes, M., & Guttorp, P. (2010). Handbook of spatial statistics. CRC Press. |
| [25] | Bhutta, Z. A., Das, J. K., Bahl, R., Lawn, J. E., Salam, R. A., Paul, V. K., Sankar, M. J., Blencowe, H., Rizvi, A., Chou, V. B., & Walker, N. (2014). Can available interventions end preventable deaths in mothers, newborn babies, and stillbirths, and at what cost? Lancet, 384(9940), 347-370. |
APA Style
Avwerhota, O. O., Avwerhota, M., Daniel, E. O., Popoola, T. A., Popoola, I. O., et al. (2024). Bayesian Spatial Analysis of Risk Factors Affecting Low Birth Weight in Nigeria. Journal of Family Medicine and Health Care, 10(3), 40-50. https://doi.org/10.11648/j.jfmhc.20241003.11
ACS Style
Avwerhota, O. O.; Avwerhota, M.; Daniel, E. O.; Popoola, T. A.; Popoola, I. O., et al. Bayesian Spatial Analysis of Risk Factors Affecting Low Birth Weight in Nigeria. J. Fam. Med. Health Care 2024, 10(3), 40-50. doi: 10.11648/j.jfmhc.20241003.11
@article{10.11648/j.jfmhc.20241003.11,
author = {Oladayo Olarinre Avwerhota and Michael Avwerhota and Ebenezer Obi Daniel and Taiwo Aderemi Popoola and Israel Olukayode Popoola and Adebanke Adetutu Ogun and Ahmed Mamuda Bello and Michael Olabode Tomori and Aisha Oluwakemi Salami and Celestine Emeka Ekwuluo and Olukayode Oladeji Alewi and Aremu Bukola Janet},
title = {Bayesian Spatial Analysis of Risk Factors Affecting Low Birth Weight in Nigeria
},
journal = {Journal of Family Medicine and Health Care},
volume = {10},
number = {3},
pages = {40-50},
doi = {10.11648/j.jfmhc.20241003.11},
url = {https://doi.org/10.11648/j.jfmhc.20241003.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.jfmhc.20241003.11},
abstract = {Low birth weight (LBW), defined by the World Health Organization as a birth weight of less than 2.5 kilograms, is a major public health concern with significant implications for neonatal morbidity, mortality, and long-term health outcomes. LBW prevalence is particularly high in developing countries, contributing to substantial healthcare challenges and socio-economic burdens. This study examines the determinants of LBW in Nigeria, focusing on socio-demographic, economic, and health-related factors. This cross-sectional study utilizes data from the 2018 Nigeria Demographic and Health Survey (NDHS). A stratified two-stage cluster sampling method was employed, and data were collected through structured interviews. The analysis included socio-demographic characteristics, economic status, health factors, and birth weights, which were classified into LBW and normal birth weight categories. Ethical approval was obtained, and informed consent ensured participant confidentiality. The analysis revealed significant associations between LBW and several factors. Higher maternal education levels were linked to lower odds of LBW. Religious affiliation also impacted LBW, with Muslim mothers having a lower likelihood of LBW compared to Christian mothers. Ethnicity influenced LBW outcomes, with Igbo mothers showing higher odds of LBW compared to Yoruba mothers. Economic stability and urban residency were associated with reduced LBW risk. Health factors such as maternal BMI and frequent antenatal visits were protective against LBW. Geographic disparities indicated higher risks in northern Nigeria. The study underscores the multifactorial nature of LBW, highlighting the importance of maternal education, socio-economic support, and healthcare access. Tailored interventions addressing ethnic and religious contexts, along with region-specific strategies, are essential. The Bayesian STAR model's superior performance suggests that spatial and non-parametric considerations provide deeper insights into LBW risk factors. Comprehensive, multifaceted strategies and policies are needed to address the determinants of LBW, focusing on vulnerable populations and regional disparities.
},
year = {2024}
}
TY - JOUR T1 - Bayesian Spatial Analysis of Risk Factors Affecting Low Birth Weight in Nigeria AU - Oladayo Olarinre Avwerhota AU - Michael Avwerhota AU - Ebenezer Obi Daniel AU - Taiwo Aderemi Popoola AU - Israel Olukayode Popoola AU - Adebanke Adetutu Ogun AU - Ahmed Mamuda Bello AU - Michael Olabode Tomori AU - Aisha Oluwakemi Salami AU - Celestine Emeka Ekwuluo AU - Olukayode Oladeji Alewi AU - Aremu Bukola Janet Y1 - 2024/08/30 PY - 2024 N1 - https://doi.org/10.11648/j.jfmhc.20241003.11 DO - 10.11648/j.jfmhc.20241003.11 T2 - Journal of Family Medicine and Health Care JF - Journal of Family Medicine and Health Care JO - Journal of Family Medicine and Health Care SP - 40 EP - 50 PB - Science Publishing Group SN - 2469-8342 UR - https://doi.org/10.11648/j.jfmhc.20241003.11 AB - Low birth weight (LBW), defined by the World Health Organization as a birth weight of less than 2.5 kilograms, is a major public health concern with significant implications for neonatal morbidity, mortality, and long-term health outcomes. LBW prevalence is particularly high in developing countries, contributing to substantial healthcare challenges and socio-economic burdens. This study examines the determinants of LBW in Nigeria, focusing on socio-demographic, economic, and health-related factors. This cross-sectional study utilizes data from the 2018 Nigeria Demographic and Health Survey (NDHS). A stratified two-stage cluster sampling method was employed, and data were collected through structured interviews. The analysis included socio-demographic characteristics, economic status, health factors, and birth weights, which were classified into LBW and normal birth weight categories. Ethical approval was obtained, and informed consent ensured participant confidentiality. The analysis revealed significant associations between LBW and several factors. Higher maternal education levels were linked to lower odds of LBW. Religious affiliation also impacted LBW, with Muslim mothers having a lower likelihood of LBW compared to Christian mothers. Ethnicity influenced LBW outcomes, with Igbo mothers showing higher odds of LBW compared to Yoruba mothers. Economic stability and urban residency were associated with reduced LBW risk. Health factors such as maternal BMI and frequent antenatal visits were protective against LBW. Geographic disparities indicated higher risks in northern Nigeria. The study underscores the multifactorial nature of LBW, highlighting the importance of maternal education, socio-economic support, and healthcare access. Tailored interventions addressing ethnic and religious contexts, along with region-specific strategies, are essential. The Bayesian STAR model's superior performance suggests that spatial and non-parametric considerations provide deeper insights into LBW risk factors. Comprehensive, multifaceted strategies and policies are needed to address the determinants of LBW, focusing on vulnerable populations and regional disparities. VL - 10 IS - 3 ER -
Department of Public Health, Atlantic International University, Hawaii, United States of America
Department of Public Health, Swansea University, Swansea, United Kingdom; Department of Public Health, Texila American University, Georgetown, Guyana
Department of Research, Smartnovation Limited, Birmingham United Kingdom
Department of Epidemiology and Community Health, University of Ilorin, Ilorin, Nigeria
Department of Policy, Governance, Liaison, and Support, International Organization for Migration, Abuja, Nigeria
Department of Public Health, Texila American University, Georgetown, Guyana
Department of Public Health, Texila American University, Georgetown, Guyana
Department of Public Health, Texila American University, Georgetown, Guyana
Department of Health and Nutrition Sector, International Medical Corps, Kyiv, Ukraine
Department of Public Health, Texila American University, Georgetown, Guyana
Department of Public Health, Texila American University, Georgetown, Guyana
Information