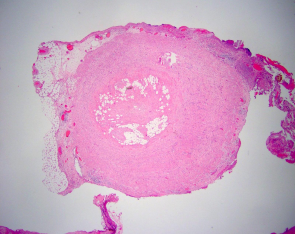
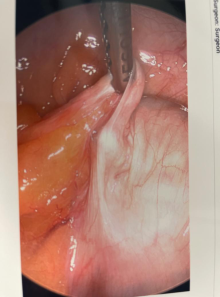
Acute appendicitis is the most common appendiceal disease, however, there are some chronic inflammatory disease pathologies such as appendiceal obliterans (AO) that mimic acute appendicitis. We present a five-year retrospective case series analysis in a community hospital for patients who underwent appendectomy. Fibrous obliteration of the appendix occurs when there is a replacement of the mucosa and submucosa with fibrotic tissues. In a small community hospital, there were 195 patients that underwent appendectomy within a five-year period, in which 6.66% of patients' final pathology confirmed AO. There are some similar clinical symptoms and computed tomography (CT) findings of AO that can mimic acute appendicitis, but there is no consensus for any criteria to definitively diagnose this condition radiologically. The current method to determine the etiology of this appendiceal condition is through appendectomy followed by histological evaluation by a pathologist. We aim to analyze prior patients and their risk factors to find an alternative diagnostic method. We explore several factors including age, to determine if there can be any basis to creating a diagnostic criterion for this condition. The mean age within our case series was 58 years old. While fibrous obliteration of the appendix is a chronic inflammatory process, patients may present with acute abdominal pain, making the diagnosis difficult. Therefore, clinicians should make AO a part of their differential diagnosis which may require surgical intervention.
| Published in | World Journal of Medical Case Reports (Volume 5, Issue 2) |
| DOI | 10.11648/j.wjmcr.20240502.11 |
| Page(s) | 18-22 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Fibrous Obliteration, Appendiceal Obliterans, Appendectomy, Acute Appendicitis, Neuroendocrine, Pathology, General Surgery
Case number | Age | Sex | Symptoms/Indications | CTAP | Surgical modality | Type of surgery |
|---|---|---|---|---|---|---|
1 | 50 | M | Colonic mass | no | Lap | Lap assisted right hemicolectomy |
2 | 83 | F | Abdominal pain, vomiting, constipation --> small bowel obstruction | CT | Lap, converted Expolartory-lap, open | Diagnostic laparoscopy |
3 | 75 | F | Elective reversal of colostomy | no | Lap | Appendectomy |
4 | 28 | F | RLQ pain | no | Lap | Appendectomy |
5 | 44 | F | Congenital intestinal malrotation | no | Lap | Appendectomy* |
6 | 59 | F | Abdominal pain -> perforated sigmoid, diverticulosis, acute peritonitis | no | Lap | Diagnostic laparoscopy, Hartmann’s |
7 | 56 | M | Toxic megacolon | no | Lap | Appendectomy, cecostomy tube placement |
8 | 67 | F | Perforated viscus | CT | Lap | Partial cecotomy, appendectomy |
9 | 78 | F | Colonic mass | CT | Lap | Right colectomy |
10 | 83 | F | Abdominal pain | CT | Lap | Laparoscopic colon resection, appendectomy, colostomy |
11 | 55 | M | N/V/D, RLQ pain | CT | Lap | Appendectomy |
12 | 34 | F | RLQ Pain Nausea | CT | Lap | Diagnostic laparoscopy, LOA, Appendectomy |
13 | 39 | F | RLQ pain | CT | Lap | Appendectomy |
AO | Appendiceal Obliterans |
CT | Computerized Tomography |
VIP | Vasoactive Intestinal Peptide |
| [1] | Olsen, B. S., & Holck, S. (1987). Neurogenous hyperplasia leading to appendiceal obliteration: an immunohistochemical study of 237 cases. Histopathology, 11(8), 843–849. |
| [2] | Leibovitch, I., Avigad, I., Nativ, O., & Goldwasser, B. (1992). The frequency of histopathological abnormalities in incidental appendectomy in urological patients: the implications for incorporation of the appendix in urinary tract reconstruction. The Journal of urology, 148(1), 41–43. |
| [3] | Petroianu, A., Barroso, T. V. V., Buzelin, M. A., Theobaldo, B. M., & Tafuri, L. S. A. (2020). Neuroendocrine apendicopathy in morphologically normal appendices of patients with diagnosis of acute appendicitis: Diagnostic study. Annals of medicine and surgery (2012), 60, 344–351. |
| [4] | Li Y, Li M, Li X, Sang H. Metastasis to the appendix from adenocarcinoma of the ascending colon: A case report. Medicine (Baltimore). 2017 Mar; 96(11): e6357. |
| [5] | Dincel O, Göksu M, Türk BA, Pehlivanoğlu B, İşler S. Incidental Findings in Routine Histopathological Examination of Appendectomy Specimens; Retrospective Analysis of 1970 Patients. Indian J Surg. 2018 Feb 80(1): 48-53. |
| [6] | Sarathy KR, Samee A (2021) Pristine Normal Looking Appendix on Diagnostic Laparoscopy-A Management Dilemma. Int J Surg Res Pract 8: 135. |
| [7] | Choi, Sun-Ju & Jang, Yun-Jin & Lee, Dakeun & Cho, S. & Kim, Gab & Bae, Ji & Park, Jin & Cheon, Jae. (2014). Two Cases of Fibrous Obliteration of the Appendix, Mimicking Acute Appendicitis. Journal of the Korean Society of Radiology. 70. 430. |
| [8] | Joseph Misdraji, Fiona M. Graeme-Cook, Miscellaneous conditions of the appendix, Seminars in Diagnostic Pathology, Volume 21, Issue 2, 2004, Pages 151-163, ISSN 0740-2570, |
| [9] |
Gonzales, R. S. (2021, April 28). Appendix - fibrous obliteration.
https://www.pathologyoutlines.com/topic/appendixfibrousobliteration.html |
| [10] | Weissleder, R., & Al, E. (2011). Primer of diagnostic imaging (5th ed., pp.147-148). Elsevier Mosby. |
| [11] | Davis CR, Trevatt A, Dixit A, Datta V. Systematic review of clinical outcomes after prophylactic surgery. Ann R Coll Surg Engl. 2016 Jul; 98(6): 353-7. |
| [12] | Echevarria S, Rauf F, Hussain N, Zaka H, Farwa UE, Ahsan N, Broomfield A, Akbar A, Khawaja UA. Typical and Atypical Presentations of Appendicitis and Their Implications for Diagnosis and Treatment: A Literature Review. Cureus. 2023 Apr 2; 15(4): e37024. |
APA Style
Uddin, T., Aktar, M., Islam, R., Quazi, N., Wilson, A. (2024). Appendiceal Obliterans Fibrosis: A Five-Year Case Series Report in a Community Hospital. World Journal of Medical Case Reports, 5(2), 18-22. https://doi.org/10.11648/j.wjmcr.20240502.11
ACS Style
Uddin, T.; Aktar, M.; Islam, R.; Quazi, N.; Wilson, A. Appendiceal Obliterans Fibrosis: A Five-Year Case Series Report in a Community Hospital. World J. Med. Case Rep. 2024, 5(2), 18-22. doi: 10.11648/j.wjmcr.20240502.11
AMA Style
Uddin T, Aktar M, Islam R, Quazi N, Wilson A. Appendiceal Obliterans Fibrosis: A Five-Year Case Series Report in a Community Hospital. World J Med Case Rep. 2024;5(2):18-22. doi: 10.11648/j.wjmcr.20240502.11
@article{10.11648/j.wjmcr.20240502.11,
author = {Tanjil Uddin and Mohammad Aktar and Rayan Islam and Nadim Quazi and Abralena Wilson},
title = {Appendiceal Obliterans Fibrosis: A Five-Year Case Series Report in a Community Hospital
},
journal = {World Journal of Medical Case Reports},
volume = {5},
number = {2},
pages = {18-22},
doi = {10.11648/j.wjmcr.20240502.11},
url = {https://doi.org/10.11648/j.wjmcr.20240502.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.wjmcr.20240502.11},
abstract = {Acute appendicitis is the most common appendiceal disease, however, there are some chronic inflammatory disease pathologies such as appendiceal obliterans (AO) that mimic acute appendicitis. We present a five-year retrospective case series analysis in a community hospital for patients who underwent appendectomy. Fibrous obliteration of the appendix occurs when there is a replacement of the mucosa and submucosa with fibrotic tissues. In a small community hospital, there were 195 patients that underwent appendectomy within a five-year period, in which 6.66% of patients' final pathology confirmed AO. There are some similar clinical symptoms and computed tomography (CT) findings of AO that can mimic acute appendicitis, but there is no consensus for any criteria to definitively diagnose this condition radiologically. The current method to determine the etiology of this appendiceal condition is through appendectomy followed by histological evaluation by a pathologist. We aim to analyze prior patients and their risk factors to find an alternative diagnostic method. We explore several factors including age, to determine if there can be any basis to creating a diagnostic criterion for this condition. The mean age within our case series was 58 years old. While fibrous obliteration of the appendix is a chronic inflammatory process, patients may present with acute abdominal pain, making the diagnosis difficult. Therefore, clinicians should make AO a part of their differential diagnosis which may require surgical intervention.
},
year = {2024}
}
TY - JOUR T1 - Appendiceal Obliterans Fibrosis: A Five-Year Case Series Report in a Community Hospital AU - Tanjil Uddin AU - Mohammad Aktar AU - Rayan Islam AU - Nadim Quazi AU - Abralena Wilson Y1 - 2024/11/18 PY - 2024 N1 - https://doi.org/10.11648/j.wjmcr.20240502.11 DO - 10.11648/j.wjmcr.20240502.11 T2 - World Journal of Medical Case Reports JF - World Journal of Medical Case Reports JO - World Journal of Medical Case Reports SP - 18 EP - 22 PB - Science Publishing Group SN - 2994-726X UR - https://doi.org/10.11648/j.wjmcr.20240502.11 AB - Acute appendicitis is the most common appendiceal disease, however, there are some chronic inflammatory disease pathologies such as appendiceal obliterans (AO) that mimic acute appendicitis. We present a five-year retrospective case series analysis in a community hospital for patients who underwent appendectomy. Fibrous obliteration of the appendix occurs when there is a replacement of the mucosa and submucosa with fibrotic tissues. In a small community hospital, there were 195 patients that underwent appendectomy within a five-year period, in which 6.66% of patients' final pathology confirmed AO. There are some similar clinical symptoms and computed tomography (CT) findings of AO that can mimic acute appendicitis, but there is no consensus for any criteria to definitively diagnose this condition radiologically. The current method to determine the etiology of this appendiceal condition is through appendectomy followed by histological evaluation by a pathologist. We aim to analyze prior patients and their risk factors to find an alternative diagnostic method. We explore several factors including age, to determine if there can be any basis to creating a diagnostic criterion for this condition. The mean age within our case series was 58 years old. While fibrous obliteration of the appendix is a chronic inflammatory process, patients may present with acute abdominal pain, making the diagnosis difficult. Therefore, clinicians should make AO a part of their differential diagnosis which may require surgical intervention. VL - 5 IS - 2 ER -
Department of Medicine, New York Institute of Technology College of Osteopathic Medicine, Old Westbury, The United States
Department of Medicine, New York Institute of Technology College of Osteopathic Medicine, Old Westbury, The United States
Department of Medicine, New York Institute of Technology College of Osteopathic Medicine, Old Westbury, The United States
Department of Medicine, New York Institute of Technology College of Osteopathic Medicine, Old Westbury, The United States
General Surgery Department, Catholic Health Mercy Hospital, Rockville Centre, The United States
Information