Abstract
Objective: Rubella is a vaccine-preventable disease that is primarily unnoticed public health problem. Hence, this study aims to describe the outbreak in terms of person, place, time, guide control measures and determine risk factors associated in Lideta Sub City, Woreda-3, Addis Ababa, Ethiopia. Methods: A 1:2 unmatched case-control study was conducted from February 20, 2022, to June 10, 2022. Each rubella case was identified based on the World Health Organization standard case definition. A total of 32 cases and 64 controls were interviewed by using a structured questionnaire, then, bivariate analysis was conducted to prepare for further multivariate analysis to control all potential confounders to identify the true predictors of rubella infection, variables with a p-value <0.05 had a statistically significant association with rubella infection. Results: In the study setting, 32 rubella cases were listed in the line list and tested to laboratory confirmation. Based on the laboratory results, 1 case were inconclusive, while 11 cases laboratory tested positive for rubella IgM, with an attack rate of 2 per 1000. The current study showed that 59.4% of cases are female. In the multivariable analysis, ages between 1-2 years (AOR: 5.05, 95% CI: 1.49-17.12), undernourished children (AOR: 4.27, 95% CI: 1.38-13.17), travel history (AOR: 3.96, 95% CI: 1.34-11.76) and poor housing conditions (AOR: 4.18, 95% CI: 1.39-12.55) were significant factors associated with rubella infection. Conclusion: The outbreak was caused by the absence of a rubella surveillance system, and unvaccination against rubella which increased the transmission of rubella infection. Hence, immediate isolate and treat the sick person, functional rubella surveillance system, routine rubella vaccination for susceptible childbearing women, vaccination of infants, or a combined strategy could prevent similar outbreaks.
Keywords
Rubella Outbreak, Outbreak Investigation, Lideta Sub-city, Woreda 3
1. Introduction
Rubella is an infectious disease caused by an enveloped RNA virus belonging to the Rubivirus genus within the Togaviridae family. It is transmitted through the respiratory route and initially replicates in the nasopharyngeal mucosa and local lymph nodes. Transmission from person to person occurs via direct or droplet contact with nasopharyngeal secretions shed from infected individuals. Furthermore, rubella can be transmitted by individuals with subclinical or asymptomatic infections, accounting for up to 50% of all rubella cases. The rash typically lasts for one to three days and is fainter than a measles rash. It does not coalesce (merge) and may be difficult to detect on pigmented skin. The incubation period for the rubella virus is 14 days, with a range of 7 to 21 days
.
Globally, an estimated 100,000 cases of congenital rubella syndrome (CRS) occur each year. In developing countries, the annual incidence of CRS is estimated at 110,000 cases, with a range of 14,000 to 308,000. Up to 90% of infants born to mothers infected with rubella during the first trimester will develop physical anomalies, referred to as CRS. Consequently, countries with high prevalence rates of rubella susceptibility among women of childbearing age are at the highest risk of CRS. This risk varies between countries due to epidemiological and socioeconomic differences
.
Almost all African countries have not yet established rubella control or elimination goals. A recent study conducted in Kuyu District, Ethiopia, reported 49 cases of rubella, with 50.1% of the cases occurring in females. Previous studies conducted in Zimbabwe identified contact history exposure to rubella and family size (more than three children in the household) as risk factors for rubella infection. Another similar study conducted in Addis Ababa, Ethiopia, showed that 55.2% of the rubella cases were in females, and 77.59% of the cases were among children aged 3-5 years
.
In Ethiopia, a dedicated rubella surveillance system is not yet established. However, rubella cases have been identified through the measles surveillance system. These cases were initially suspected as measles, but they tested negative for measles IgM antibodies. Subsequent testing for rubella IgM antibodies confirmed the presence of rubella
. Due to the absence of a dedicated rubella surveillance system in Ethiopia, the 2022 PHEM database showed a suspected measles outbreak, despite no recorded rubella outbreak. This study aims to provide valuable information to stakeholders and policymakers, and identify the characteristics of a potential rubella outbreak in terms of person, place, time, and risk factors in Lideta sub-city, Woreda-3, Addis Ababa, Ethiopia, during 2022.
2. Methods
2.1. Study Area
This study was carried out in Lideta sub-city, Woreda-3, Addis Ababa, Ethiopia. According to population projections from 2017, the woreda population is 51,092, with 26,567 females. There are 1,167 children under one year old and 3,733 children under five years old. The woreda is served by one health center, one private general hospital, three medium clinics, and three primary clinics.
2.2. Study Design and Period
A descriptive 1:2 unmatched case-control study was conducted from February 20, 2022, to June 10, 2022.
2.3. Data Collection Tool and Sampling
This rubella outbreak investigation involved 32 cases and 64 controls. Each case was entered into a line list, and a house-to-house search was conducted to select controls. Controls were chosen from two neighbors residing in the same kebele and in close proximity to a confirmed rubella case. Based on the caseload, the questionnaire was allocated to the chosen kebele. Data was gathered using the Kobo Data collection tools through in-person interviews. To maximize the response rate, a systematic chronological ordering of sensitive questions was employed. The questionnaire included socio-demographic data for both cases and controls, clinical presentation data for cases only, treatment information for cases only, potential risk factors for cases and controls, immunization status, and immunization information for both cases and controls.
2.4. Operational Definition
Rubella case: Rubella case was defined as a laboratory-confirmed case of a suspected case with a positive blood test for rubella-specific IgM plus a patient with a febrile rash illness that is linked to contact with laboratory-confirmed rubella case. Finally, a total of 29 questions were used to measure the composite scale to assess the rubella outbreak investigation.
A confirmed rubella outbreak is defined as the occurrence of three or more confirmed rubella cases (at least two of which should be laboratory confirmed; IgM positive) in a health district (approximate catchment population of 100,000) in a month.
Epidemiologically confirmed rubella case: a patient had febrile rash illness that is linked epidemiologically to a laboratory confirmed rubella case.
Woreda/Kebele: the smallest administrative unit in Ethiopia.
2.5. Inclusion Criteria
Case: any person resident in Lideta sub city woreda-3, catchment that tested positive for IgM or a person who had fulfill WHO standard case definition during the study period.
Control: Any person residents in the Lideta sub city woreda-3, catchment during the study period who did not develop signs and symptoms of rubella infection with willing to participate included in the study.
2.6. Exclusion Criteria
Cases: those cases did not fulfill the WHO rubella case definition and were excluded from the study.
Controls: those persons who had unable to communicate and do not live at home during interviewing period.
2.7. Variable in the Study
Socio demographic variable: sex case and control, Age of case and control in year, respondent relation to case (Mather, Father, Sibling others), Occupation of parents, educational level of cases and control, educational level of parents, Weight in kg, Height in meter.
Clinical presentation only for case: Sign and symptom, onset of rash, Complication, service delivery point, date of admission, pregnancy status.
Treatment information only for case: Health facility seen, date of health facility seen, Received treatment, Types of treatment, isolation status, treatment outcome
Risk factors: similar sign symptom in the family, contact history, travel history, place of travel, how many person live in house hold, number of rooms, Number of windows, room well illuminated, area of home in meter square (m2) and house condition.
2.8. Data Quality Control
The rubella case definition was clearly defined based on the WHO standard case definition to minimize misclassification bias
. Both cases and controls were registered during the data collection period. Data quality assurance was ensured by providing two full days of training to data collectors and supervisors, accompanied by a training manual. A 10% pre-test was conducted on a similar population in a non-selected woreda in Lideta sub-city, Addis Ababa, Ethiopia, to identify potential problems and minimize information bias related to interviewer misclassification, recall bias, and inter- and intra-observer bias. Finally, data validity and reliability were maintained through close supervision of data collectors by the principal investigator.
2.9. Data Processing and Analysis
The data was collected and entered into the Kobo Toolbox, then exported to SPSS version 25 for analysis. All covariates with a p-value < 0.2 were selected as criteria during bivariate analysis to control for potential confounders and identify true predictors of the outbreak. Variables with a p-value <0.05 in multivariate analysis were considered significant predictors of the outbreak. Odds ratios, along with 95% confidence intervals, were estimated to measure the association level and statistical significance, declared at a p-value < 0.05. Finally, the study findings were summarized using narrative text, tables, and graphs.
3. Results
3.1. Descriptive Epidemiology
In the current study, 32 cases and 64 controls were planned for interviews, resulting in a 100% response rate. Of the total tested rubella cases, one case was inconclusive, while 11 cases were IgM positive. The remaining cases were epidemiologically linked to confirmed rubella cases. This outbreak began on February 20, 2022, reached its peak on March 10, 2022, and subsided on April 10, 2022. Approximately 59.4% of the cases were female. The overall attack rate for rubella cases was 2 per 1000, with a higher attack rate reported among children aged 5 years and older (2.1 per 1000). All cases were treated in the outpatient department (
Table 1).
Table 1. Age specific attack rate of the Rubella outbreak in Lideta sub city Abinet heath center Addis Ababa Ethiopia.
SN | Age category by year | Rubella cases | Population at risk | Attack rate AR/1000 |
1 | 1-2 | 12 | 1143 | 1.74 |
2 | 3-4 | 2 | 3713 | 1.62 |
3 | ≥5 | 18 | 17699 | 2.1 |
Total | 32 | 22555 | 2 |
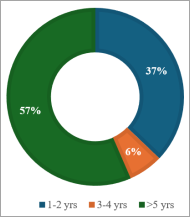
The outbreak affected six Kebeles in the woreda, with the highest number of cases observed in Kebeles 26, 36, and 27, accounting for 31%, 28%, and 13% of the total cases, respectively. Regarding the rubella outbreak, children aged 1-2 years were the most affected age group in the current outbreak (37%) compared to children aged 3-4 years (6.25%) (
Figure 1).
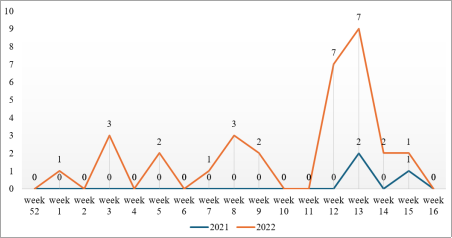
The first suspected cases were reported on February 20, 2022, from Kebele 26. The epidemic curve shows multiple peaks, indicating a propagated type of transmission. The outbreak reached its peak between March 10 and 20, 2022. No cases were reported after April 21, 2022 (
Figure 2).
Figure 1. Rubella cases by age in Lideta sub city woreda-3, Addis Ababa city, Ethiopia, 2022.
Figure 2. Rubella cases by WHO Epi-week in Lideta sub city woreda-3, Addis Ababa, Ethiopia, 2022.
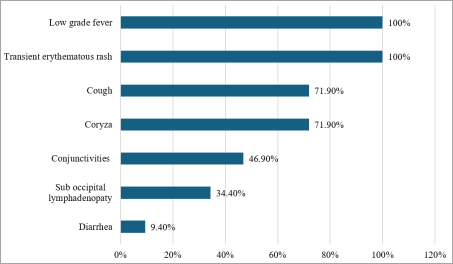
According to the findings, all cases developed rubella-like symptoms, including low-grade fever (100%), a transient erythematous rash (100%), cough (72%), Coryza (72%), conjunctivitis (47%), and diarrhea (9.38%) (
Figure 3).
Figure 3. Rubella cases by sign in Lideta sub city woreda 3, Addis Ababa, Ethiopia, 2022.
3.2. Socio Demographic Characteristic
A descriptive 1: 2 unmatched case-control study was conducted with a total of 32 cases and 64 controls. The mean age of the cases was 2.19 years (SD ±0.965), and the mean age of the controls was 2.59 years (SD ±0.750). Regarding age category, approximately 37% of cases and 15.6% of controls were aged between 1 and 2 years. Almost 59.4% of the cases and 56.3% of the controls were female. Approximately 56.3% of cases and 35.9% of controls had poor housing conditions. Regarding travel history, 46.9% of cases and 31.3% of controls reported a history of travel (
Table 2).
Table 2. Socio-demographic factors of the study participant in Lideta sub city, woreda-3, Addis Ababa city, Ethiopia, 2022.
Variable | Respondent status |
Case (N=32) | Control (N=64) |
Sex |
Male | 13 (40.6%) | 28 (43.8) |
Female | 19 (59.4%) | 36 (56.3%) |
Age |
1-2 | 12 (37.5%) | 10 (15.6%) |
3-4 | 2 (6.3%) | 6 (9.4%) |
≥ 5 | 18 (56.3%) | 48 (75%) |
Body Mass Index |
13-17 | 23 (71.9%) | 28 (43.8%) |
18-24 | 1 (3.1%) | 4 (6.3%) |
≥ 25 | 8 (25%) | 32 (50%) |
Contact History |
Yes | 28 (87.5%) | 44 (68.8%) |
No | 4 (12.5%) | 20 (31.3%) |
Travel History |
Yes | 17 (46.9%) | 20 (31.3%) |
No | 15 (53.1%) | 44 (68.8%) |
House Condition |
Ventilated | 14 (43.8%) | 41 (64.1%) |
Not ventilated | 18 (56.3%) | 23 (35.9%) |
3.3. Multivariate Analysis
All variables selected during bivariate analysis were entered into a multivariate logistic regression model to identify independent predictors of rubella infection. Children aged 1-2 years were 5.1 times more likely to contract rubella infection (AOR: 5.1, 95% CI: 1.49-17.12) than children aged 5 years and older, undernourished children were 4.27 times more likely to contract rubella infection (AOR: 4.27, 95% CI: 1.38-13.17) than those with good nutritional status, children with a history of travel were 3.96 times more likely to be infected with rubella (AOR: 3.96, 95% CI: 1.34-11.73) compared to those without a travel history, and children living in houses without adequate ventilation were 4.181 times more likely to be infected with rubella (AOR: 4.181, 95% CI: 1.392-12.55) compared to those living in well-ventilated houses (
Table 3).
Table 3. Multivariable analysis of factors associated with the rubella outbreak in Lideta sub-city, woreda-3, Addis Ababa, Ethiopia, 2022.
Variable | Respondent status | COR (95% CI) | AOR (95% CI) |
Case (N=32) | Control (N=64) |
Age of respondent |
1-2 | 12 (37.5%) | 10 (15.6% | 2.968(1.08, 8.021) | 5.052(1.491,17.120) * |
3-4 | 2 (6.3%) | 6 (9.4%) | 0.829(0.153, 4.45) | 0.546(0.079, 3.757) |
> 5 | 18 (56.3%) | 48 (75.0%) | 1 | 1 |
Body Mass Index |
13-17 | 23 (71.9%) | 28 (43.3%) | 2.289(1.122, 7.183) | 4.267(1.382, 13.17) * |
18-24 | 1 (3.1%) | 4 (6.3%) | 0.85(0.85, 8.706) | 0.559(0.042, 7.429) |
> 25 | 8 (25%) | 32 (50.0%) | 1 | 1 |
Contact History |
Yes | 28 (87.5%) | 44 (68.8%) | 3.372(1.044, 10.89) | 2.635(0.722, 9.615) |
No | 4 (12.5%) | 20 (31.3%) | 1 | 1 |
Travel History |
Yes | 17 (53.1%) | 20 (31.3%) | 2.779(1.63, 6.641) | 3.963(1.339, 11.73) * |
No | 15 (46.9%) | 44 (68.8%) | 1 | 1 |
House Condition |
Ventilated | 14 (43.8%) | 41 (64.1%) | 1 | 1 |
Not Ventilated | 18 (56.3%) | 23 (35.9%) | 2.529(1.067, 5.99) | 4.181(1.392, 12.55) * |
Abbreviations: AOR: Adjusted Odd Ratio, CI: Confidence Interval, COR: Crude Odd Ratio.
4. Discussion
According to this study, children aged 1-2 years, those with poor nutritional status, a history of travel, and those living in poorly ventilated homes were predisposing factors for rubella infection transmission in Ethiopia. The strongest driving factors for rubella infection transmission were undernourished children and poor household ventilation. This may be attributed to the lack of a dedicated rubella outbreak surveillance system and the absence of a national rubella immunization program in Ethiopia, making many Ethiopian children susceptible to rubella infection.
This study demonstrated that a higher proportion of rubella infections were observed in females. Further investigation is needed to better understand the underlying factors contributing to this disparity in infection rates between sexes. The study also showed that higher attack rates were reported among children aged 1-2 years. This finding is consistent with previous studies conducted in Kuyu District, Ethiopia, and Yea Sub-city, Addis Ababa, Ethiopia
. This may be due to the fact that young children have not yet acquired immunity to rubella, while older individuals may have acquired immunity from prior exposure, making them resistant to infection.
Children with a history of travel in the affected area were 3.96 times more likely to acquire rubella infection than those without a travel history. This finding is consistent with a study conducted in Gokwe North District, Midland province, Zimbabwe
. This study also demonstrated that a higher proportion of rubella infections were observed in children aged 1-2 years compared to those aged 5 years and older. This finding contrasts with earlier studies conducted in Addis Ababa, Ethiopia
. This suggests that having a travel history in the affected area increases the risk of coming into contact with an infected individual.
Another interesting finding of this study showed that children living in poor household conditions were 4.18 times more likely to experience rubella infection transmission than those living in good household conditions. This finding is consistent with a study conducted in Kuyu District, Ethiopia
. Another interesting finding was that undernourished children were significantly associated with rubella infection. This may be attributed to the direct relationship between rubella infection transmission and poor household conditions and malnutrition factors.
5. Conclusion and Recommendation
Multivariate analysis revealed that children aged 1-2 years, those with a history of travel, undernourished children, and those living in poor household conditions were significantly associated with rubella infection. The outbreak was likely driven by a combination of poor environmental conditions, lack of routine rubella vaccination for susceptible populations, and the absence of a robust rubella surveillance system, all of which contributed to increased transmission of rubella infection. Therefore, to prevent future outbreaks, a multifaceted approach is recommended, including: Early isolation and treatment of individuals with suspected rubella infection, Establishment of a national rubella surveillance system, Implementation of routine rubella vaccination programs for susceptible women and infants with consideration of a combined strategy that addresses all these elements. Furthermore, provide valuable information to stakeholder’s policymakers, like Ethiopian Public Health Institute, Addis Ababa Regional Health Bureau-Public Health Research and Emergency Management Directorate, and World Health Organization.
6. Limitation
This study employed a retrospective interview method, which may have introduced recall bias. To minimize this potential bias, the authors endeavored to shorten the time between the onset of illness and data collection. While the sample size met the minimum requirements determined by the sample size calculation, it remained relatively small. This explains the wide confidence intervals observed in the analysis. Finally, the cross-sectional study design limits the extent to which causality can be established and distinguishes risk factors from consequences of rubella infection.
Abbreviations
AARHB | Addis Ababa Regional Health Bureau |
EPHI | Ethiopia Public Health Institution |
FMOH | Federal Ministry of Health |
PHEM | Public Health Emergency Management |
WHO | World Health Organization |
Acknowledgments
First of all, I would like to thanks Lideta sub-city health office for provide me ethical letter. I would like to acknowledge Dr. Teshome Gebresenbet form World Health Organization and Mr. Getachew Asefa form Abinet Health Center Medical Director for supported me. Last but not the least greatly thanks Lideta sub-city woreda 3 Abinet Health Center administrators and health professionals who had help me during the study period.
Author Contributions
Anteneh Wondimagegn Assefa: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Visualization, Writing original draft.
Aklilu Negash Gudissa: Conceptualization, Writing original draft.
Siyene Yirgalem: Supervision, Writing review & editing
Mohammed Hassen: Writing review & editing.
Ethical Approval and Consent to Participant
Ethical clearance was obtained from the research and ethical committee of Lideta sub-city health office by approval letter No. L/S/C/H/O/895/22. Then a formal letter that explains the objectives, rationale and expected outcomes of the study will be written to the study area Lideta sub-city woreda-3 Abinet Health Center. Individuals younger than the age of 16 the parents/guardian informed about the purpose of the study and option of withdrawing from the study whenever they feel any discomfort and want to refuse for any reason at any time without any consequence. Finally, any information recorded anonymously and confidentiality was assured throughout the study period.
Reviewer Comment
Fortify the submission in the discussion with related literature.
Availability of Data and Materials
In this study, the data was engaged wannabe available from the corresponding author upon reasonable request.
Consent for Publication
The author declares that not consent to publication.
Funding
The authors were not supported by any funding grant.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Annamercy C Makoni. Rubella outbreak investigation, Gokwe North District, Midlands’s province, Zimbabwe, 2014-a case control study. 2015: 2-3:
https://doi.org/10.11604/pamj.2015.22.60.5939
|
| [2] |
Pediatrics A Pediatrics. Rubella Basic Epidemiology. 2022: 289.
https://www.thelancet.com/article/S0140-6736
|
| [3] |
Getachew D. Rubella outbreak in the school children, Addis Ababa, Ethiopia: February-April 2018. 2019: 1-3.
https://doi.org/10.1186/s12879-019-3873-y
|
| [4] |
Ian N. Rubella outbreak in a Rural Kenyan District, 2014: documenting the need for routine rubella immunization in Kenya. 2015: 1:
https://doi.org/10.1186/s12879-015-0989
|
| [5] |
Lambert et al. Rubella. 2016: 4-5. 2297-2307.
https://doi.org/10.1016/S0140-6736(14)60539-0
|
| [6] |
Abdulbari A. Risk Factors for Rubella Transmission in Kuyu District, Ethiopia, 2018: A Case-Control Study. 2019: 4.
https://doi.org/10.1155/2019/4719636
|
| [7] |
Dinede et al. Rubella outbreak in the school children, Addis Ababa, Ethiopia: February-April 2018. 2019: 5.
https://doi.org/10.1186/s12879-019-3873-y
|
| [8] |
World Health Organization. Measles and rubella surveillance &outbreak investigation guidelines. 2009: 6-7.
https://iris.who.int/bitstream/handle/10665/205481/B4314
|
Cite This Article
-
APA Style
Assefa, A. W., Gudissa, A. N., Yirgalem, S., Hassen, M. (2025). A Case-control Study Undertaken to Investigate a Rubella Outbreak in Lideta Sub City Woreda-3 Addis Ababa, Ethiopia. American Journal of Nursing and Health Sciences, 6(2), 26-32. https://doi.org/10.11648/j.ajnhs.20250602.12
 Copy
|
Copy
|
 Download
Download
ACS Style
Assefa, A. W.; Gudissa, A. N.; Yirgalem, S.; Hassen, M. A Case-control Study Undertaken to Investigate a Rubella Outbreak in Lideta Sub City Woreda-3 Addis Ababa, Ethiopia. Am. J. Nurs. Health Sci. 2025, 6(2), 26-32. doi: 10.11648/j.ajnhs.20250602.12
Copy
|
Download
AMA Style
Assefa AW, Gudissa AN, Yirgalem S, Hassen M. A Case-control Study Undertaken to Investigate a Rubella Outbreak in Lideta Sub City Woreda-3 Addis Ababa, Ethiopia. Am J Nurs Health Sci. 2025;6(2):26-32. doi: 10.11648/j.ajnhs.20250602.12
Copy
|
Download
-
@article{10.11648/j.ajnhs.20250602.12,
author = {Anteneh Wondimagegn Assefa and Aklilu Negash Gudissa and Siyene Yirgalem and Mohammed Hassen},
title = {A Case-control Study Undertaken to Investigate a Rubella Outbreak in Lideta Sub City Woreda-3 Addis Ababa, Ethiopia
},
journal = {American Journal of Nursing and Health Sciences},
volume = {6},
number = {2},
pages = {26-32},
doi = {10.11648/j.ajnhs.20250602.12},
url = {https://doi.org/10.11648/j.ajnhs.20250602.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajnhs.20250602.12},
abstract = {Objective: Rubella is a vaccine-preventable disease that is primarily unnoticed public health problem. Hence, this study aims to describe the outbreak in terms of person, place, time, guide control measures and determine risk factors associated in Lideta Sub City, Woreda-3, Addis Ababa, Ethiopia. Methods: A 1:2 unmatched case-control study was conducted from February 20, 2022, to June 10, 2022. Each rubella case was identified based on the World Health Organization standard case definition. A total of 32 cases and 64 controls were interviewed by using a structured questionnaire, then, bivariate analysis was conducted to prepare for further multivariate analysis to control all potential confounders to identify the true predictors of rubella infection, variables with a p-value Results: In the study setting, 32 rubella cases were listed in the line list and tested to laboratory confirmation. Based on the laboratory results, 1 case were inconclusive, while 11 cases laboratory tested positive for rubella IgM, with an attack rate of 2 per 1000. The current study showed that 59.4% of cases are female. In the multivariable analysis, ages between 1-2 years (AOR: 5.05, 95% CI: 1.49-17.12), undernourished children (AOR: 4.27, 95% CI: 1.38-13.17), travel history (AOR: 3.96, 95% CI: 1.34-11.76) and poor housing conditions (AOR: 4.18, 95% CI: 1.39-12.55) were significant factors associated with rubella infection. Conclusion: The outbreak was caused by the absence of a rubella surveillance system, and unvaccination against rubella which increased the transmission of rubella infection. Hence, immediate isolate and treat the sick person, functional rubella surveillance system, routine rubella vaccination for susceptible childbearing women, vaccination of infants, or a combined strategy could prevent similar outbreaks.},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - A Case-control Study Undertaken to Investigate a Rubella Outbreak in Lideta Sub City Woreda-3 Addis Ababa, Ethiopia
AU - Anteneh Wondimagegn Assefa
AU - Aklilu Negash Gudissa
AU - Siyene Yirgalem
AU - Mohammed Hassen
Y1 - 2025/08/15
PY - 2025
N1 - https://doi.org/10.11648/j.ajnhs.20250602.12
DO - 10.11648/j.ajnhs.20250602.12
T2 - American Journal of Nursing and Health Sciences
JF - American Journal of Nursing and Health Sciences
JO - American Journal of Nursing and Health Sciences
SP - 26
EP - 32
PB - Science Publishing Group
SN - 2994-7227
UR - https://doi.org/10.11648/j.ajnhs.20250602.12
AB - Objective: Rubella is a vaccine-preventable disease that is primarily unnoticed public health problem. Hence, this study aims to describe the outbreak in terms of person, place, time, guide control measures and determine risk factors associated in Lideta Sub City, Woreda-3, Addis Ababa, Ethiopia. Methods: A 1:2 unmatched case-control study was conducted from February 20, 2022, to June 10, 2022. Each rubella case was identified based on the World Health Organization standard case definition. A total of 32 cases and 64 controls were interviewed by using a structured questionnaire, then, bivariate analysis was conducted to prepare for further multivariate analysis to control all potential confounders to identify the true predictors of rubella infection, variables with a p-value Results: In the study setting, 32 rubella cases were listed in the line list and tested to laboratory confirmation. Based on the laboratory results, 1 case were inconclusive, while 11 cases laboratory tested positive for rubella IgM, with an attack rate of 2 per 1000. The current study showed that 59.4% of cases are female. In the multivariable analysis, ages between 1-2 years (AOR: 5.05, 95% CI: 1.49-17.12), undernourished children (AOR: 4.27, 95% CI: 1.38-13.17), travel history (AOR: 3.96, 95% CI: 1.34-11.76) and poor housing conditions (AOR: 4.18, 95% CI: 1.39-12.55) were significant factors associated with rubella infection. Conclusion: The outbreak was caused by the absence of a rubella surveillance system, and unvaccination against rubella which increased the transmission of rubella infection. Hence, immediate isolate and treat the sick person, functional rubella surveillance system, routine rubella vaccination for susceptible childbearing women, vaccination of infants, or a combined strategy could prevent similar outbreaks.
VL - 6
IS - 2
ER -
Copy
|
Download