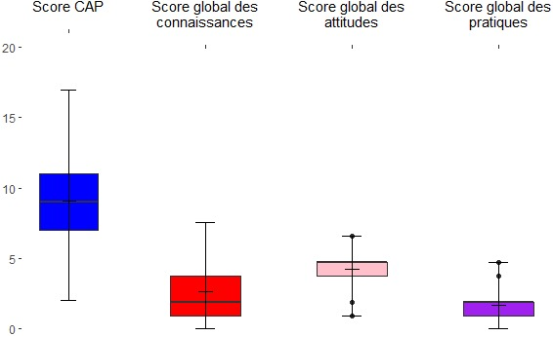
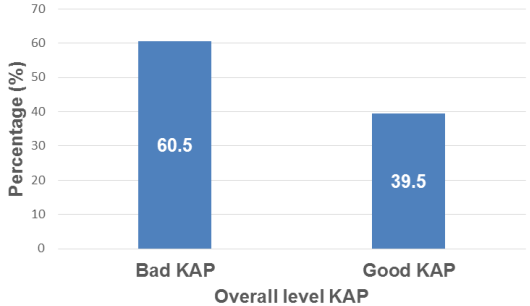
Knowledge of the relationship between pregnancy and oral health is a public health issue. The aim of this study was to assess the knowledge, attitudes and practices of pregnant women regarding oral health in the University Hospital Centers (UHC) of Ouagadougou in 2023. This was a descriptive cross-sectional study from July to September 2023. Data were collected prospectively, and knowledge, attitude and practice scores were generated. A total of 400 pregnant women were included. The [25-34] age group was the most represented at 54%, and 56.3% of women were in their 3rd trimester of pregnancy. The majority had a secondary level school and didn’t have a treating dentist. More than half (51.2%) of the respondents had poor overall knowledge of the relationship between oral health and pregnancy, 76.3% had poor attitudes and 79.5% poor practices, resulting in a poor overall KAP level for their oral health (60.5%). There was a significant variation in KAP level according to level of education (p= 0.015) and according to the information received on oral health and its implications for pregnancy (p = 0.028). Pregnant women's knowledge, attitudes and practices regarding their oral health are inadequate. Most women were unaware of the potential consequences of oral health neglect on pregnancy and their unborn child. Efforts must be made to educate them about oral health, with a focus on prevention.
| Published in | Central African Journal of Public Health (Volume 10, Issue 2) |
| DOI | 10.11648/j.cajph.20241002.17 |
| Page(s) | 116-129 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Oral Health, Pregnancy, Knowledge, Attitudes, Practices, KAP
2.1. Setting, Type and Period of Study
2.2. Study Population
2.3. Sample Size and Sampling
Structure | Number of consultations 2021* | Weight of UHC | Number of participants |
|---|---|---|---|
UHC Yalgado Ouédraogo | 2069 | 53,6% | 214 |
UHC Bogodogo | 1530 | 39.7% | 159 |
UHC Tengandogo | 258 | 6.7% | 27 |
Total | 3857 | 100% | 400 |
2.4. Data Collection Techniques and Tools
2.5. Data Processing and Analysis
2.6. Ethical and Deontological Aspects
3.1. Socio-Demographic Characteristics
Variables/ modalities | Number (n=400) | Percentage (%) | |
|---|---|---|---|
Age | |||
[18-24] | 105 | 26,3 | |
[25-34] | 216 | 54 | |
[35-44] | 78 | 19,5 | |
[45-51] | 1 | 0,3 | |
Parity | |||
0 | 102 | 25,5 | |
1 | 106 | 26,5 | |
More than one | 192 | 48 | |
Gestational age (WA) | |||
12 | 39 | 9,8 | |
[12-28] | 136 | 34 | |
≥28 | 225 | 56,3 | |
Marital status | |||
Single | 31 | 7,8 | |
Divorced/separated | 3 | 0,8 | |
Married / common-law | 366 | 91,5 | |
Study level | |||
Out of school | 102 | 25,5 | |
Primary | 60 | 15 | |
Secondary | 170 | 42,5 | |
Superior | 68 | 17 | |
Socio-professional category | |||
Tradeswoman/independent | 169 | 42,3 | |
Student | 45 | 11,3 | |
Housewife | 125 | 31,3 | |
Employee | 61 | 15,3 | |
Do you have a treating dentist? | |||
No | 389 | 97,3 | |
Yes | 11 | 2,8 | |
Since you've been pregnant, has anyone talked to you about oral health and its implications for pregnancy? | |||
No | 369 | 92,3 | |
Yes | 31 | 7,8 | |
Who gave you the information? | |||
Dental surgeon | 1 | 3,2 | |
TV show | 2 | 6,5 | |
Waiter | 1 | 3,2 | |
Gynecologist | 5 | 16,1 | |
Doctor | 3 | 9,7 | |
Midwife | 19 | 61,3 | |
3.2. Knowledge of the Relationship Between Oral Health and Pregnancy
Variables/modalities | Number (n=400) | Percentage (%) | |
|---|---|---|---|
Does pregnancy have an impact on the oral environment? | |||
Poor knowledge (no) | 259 | 64,8 | |
Good knowledge (yes) | 141 | 35,3 | |
Can pregnancy contribute to tooth gnawing (dental erosion)? | |||
Poor knowledge (no) | 322 | 80,5 | |
Good knowledge (yes) | 78 | 19,5 | |
Do pregnancy hormones provoke to gum bleeding? | |||
Poor knowledge (yes) | 277 | 69,3 | |
Good knowledge (no) | 123 | 30,8 | |
Can hormonal changes increase the risk of tooth decay during pregnancy? | |||
Poor knowledge (no) | 319 | 79,8 | |
Good knowledge (yes) | 81 | 20,3 | |
Can oral health influence pregnancy? | |||
Poor knowledge (no) | 219 | 54,8 | |
Good knowledge (yes) | 181 | 45,3 | |
Can poor oral hygiene have an impact on the course of pregnancy and lead to adverse outcomes (pre-eclampsia, low birth weight, premature delivery, stillbirth)? | |||
Poor knowledge (no) | 275 | 68,8 | |
Good knowledge (yes) | 125 | 31,3 | |
Is it possible to consult your dentist throughout your pregnancy? | |||
Poor knowledge (no) | 99 | 24,8 | |
Good knowledge (yes) | 301 | 75,3 | |
Is it possible to have dental extractions while pregnant? | |||
Poor knowledge (no) | 315 | 78,8 | |
Good knowledge (yes) | 85 | 21,3 | |
Global knowledge | |||
Poor knowledge | 205 | 51,2 | |
Good knowledge | 195 | 48,8 | |
3.3. Oral Health Attitudes During Pregnancy
Variables/modalities | Number (n=400) | Percentage (%) | |
|---|---|---|---|
Do you think you should consult a doctor if you feel pain in your mouth? | |||
Bad attitude (no) | 9 | 2,3 | |
Good attitude (yes) | 391 | 97,8 | |
Do you think you should brush your teeth morning and night for good oral hygiene? | |||
Bad attitude (no) | 4 | 1 | |
Good attitude (yes) | 396 | 99 | |
Do you think that, in addition to a toothbrush, you need to use other materials for good oral hygiene? | |||
Bad attitude (no) | 168 | 42 | |
Good attitude (yes) | 232 | 58 | |
Do you think it's necessary to change your oral hygiene habits during pregnancy? | |||
Bad attitude (no) | 182 | 45,5 | |
Good attitude (yes) | 218 | 54,5 | |
Do you think it's necessary to change your eating habits during pregnancy? | |||
Bad attitude (no) | 80 | 20 | |
Good attitude (yes) | 320 | 80 | |
Do you think it's normal to lose a tooth during pregnancy? | |||
Bad attitude (yes) | 364 | 91 | |
Good attitude (no) | 36 | 9 | |
Do you think it's necessary to have a regular dentist during pregnancy? | |||
Bad attitude (no) | 185 | 46,3 | |
Good attitude (yes) | 215 | 53,8 | |
Global attitudes | |||
Bad attitude | 305 | 76,6 | |
A good attitude | 95 | 23,8 | |
3.4. Oral Health Practices During Pregnancy
Variables/modalities | Number (n=400) | Percentage (%) | |
|---|---|---|---|
What do you do if you feel pain in your mouth? | |||
Bad practice (other) | 215 | 53,8 | |
Good practice (consult dentist) | 185 | 46,3 | |
How often do you brush your teeth? | |||
Bad practice (other) | 55 | 13,8 | |
Good practice (at least twice) | 345 | 86,3 | |
In addition to your toothbrush, do you use any other equipment to clean your teeth? | |||
Bad practice (no) | 301 | 75,3 | |
Good practice (yes) | 99 | 24,8 | |
Have you changed your oral hygiene habits? | |||
Bad practice (no) | 328 | 82 | |
Good practice (yes) | 72 | 18 | |
Have you or will you consult a dentist during pregnancy? | |||
Bad practice (no) | 385 | 96,3 | |
Good practice (yes) | 15 | 3,8 | |
Global practices | |||
Bad practice | 318 | 79,5 | |
Good practice | 82 | 20,5 | |
Variables/modalities | Overall level KAP | p-value | ||
|---|---|---|---|---|
Poor KAP n= 400 (%) | Good KAP n= 400 (%) | |||
Age | 0,129 | |||
[18 à 24] | 71 (29,3) | 34 (21,5) | ||
[25 à 34] | 130 (53,7) | 86 (54,4) | ||
[35 à 44] | 40 (16,5) | 38 (24,1) | ||
[45 à 51] | 1 (0,4) | 0 (0) | ||
Parity | 0,455 | |||
0 | 67 (27,7) | 35 (22,2) | ||
1 | 63 (26) | 43 (27,2) | ||
Gestational age (SA) | 0,459 | |||
≤12 | 20 (8,3) | 19 (12) | ||
(12-24) | 83 (34,3) | 53 (33,5) | ||
≥24 | 139 (57,4) | 86 (54,4) | ||
Marital status | 0,672 | |||
Single | 21 (8,7) | 10 (6,3) | ||
Divorced/separated | 2 (0,8) | 1 (0,6) | ||
Married / common-law | 219 (90,5) | 147 (93) | ||
Study level | 0,015 | |||
Out of school | 69 (28,5) | 33 (20,9) | ||
Primary | 31 (12,8) | 29 (18,4) | ||
Secondary | 110 (45,5) | 60 (38,0) | ||
Superior | 32 (13,2) | 36 (22,8) | ||
Socio-professional category | 0,114 | |||
Tradeswoman/independent | 95 (39,2) | 74 (46,8) | ||
Student | 23 (9,5) | 22 (13,9) | ||
Housewife | 86 (35,5) | 39 (24,7) | ||
Employee | 38 (15,7) | 23 (14,6) | ||
Do you have a primary care dentist? | 0,301 | |||
No | 237 (97,9) | 152 (96,2) | ||
Yes | 5 (2,1) | 6 (3,8) | ||
Since you've been pregnant, has anyone talked to you about oral health and its implications for pregnancy? | 0,028 | |||
No | 229 (94,6) | 140 (88,6) | ||
Yes | 13 (5,4) | 18 (11,4) | ||
4.1. Knowledge of the Relationship Between Oral Health and Pregnancy
4.2. Pregnant Women's Attitudes and Practices Regarding Oral Health and Pregnancy
4.3. Relationship Between Overall Level of Knowledge Attitudes Practices (KAP) and Socio-demographic Data
| [1] |
Cabrol D, Pons J, Goffinet F. Traité d’obstétrique. Flamarion Médecine Sciences. Paris: Flamarion Médecine Sciences; 2003.
https://ulysse.univ-lorraine.fr/permalink/33UDL_INST/1ft321i/alma991004476299705596 |
| [2] | Scheutz F, Baelum V, Matee MIM, Mwangosi I. Motherhood and dental disease. Community Dent Health. juin 2002; 19(2): 67-72. |
| [3] | Laine MA. Effect of pregnancy on periodontal and dental health. Acta Odontologica Scandinavica. 1 janv 2002; 60(5): 257-64. |
| [4] | Armitage GC. Bi-directional relationship between pregnancy and periodontal disease: Relationship between pregnancy and periodontal disease. Periodontology 2000. févr 2013; 61(1): 160-76. |
| [5] | Agrawal N, Gupta N, Tewari R, Garg AK, Yadav P. Knowledge, attitude and practice of oral health care in pregnant women in North India- a cross sectional survey. University J Dent Scie. 2017; 1(3): 22-5. |
| [6] | Pirie M, Cooke I, Linden G, Irwin C. Dental manifestations of pregnancy. The Obstetrician & Gynaecologist. 2007; 9(1): 21-6. |
| [7] | D’Aversi J. Mise en place d’une consultation de prévention bucco-dentaire au cours de la grossesse: évaluation des besoins pour les patientes suivies à la MRUN en 2013 -. [France]: Université de Lorraine; 2014. |
| [8] | Bahri N, Tohidinik H, Bahri N, Iliati H, Moshki M, Darabi F. Educational intervention to improve oral health beliefs and behaviors during pregnancy a randomized-controlled trial. J Egypt Public Health Assoc. 2015; 90(2): 41-5. |
| [9] | Laczny E, Mercier T, Clement C. Santé buccodentaire : chez la femme enceinte et la femme qui allaite. Rev Sage-Femme. 2016; 15(6): 270-6. |
| [10] | Gesase N, Miranda-Rius J, Brunet-Llobet L, Lahor-Soler E, Mahande MJ, Masenga G. The association between periodontal disease and adverse pregnancy outcomes in Northern Tanzania: a cross-sectional study. Afr Health Sci. sept 2018; 18(3): 601-11. |
| [11] | Harjunmaa U, Järnstedt J, Alho L, Dewey KG, Cheung YB, Deitchler M, et al. Association between maternal dental periapical infections and pregnancy outcomes: results from a cross-sectional study in Malawi. Tropical Medicine & International Health. 2015; 20(11): 1549-58. |
| [12] | Muwazi L, Rwenyonyi CM, Nkamba M, Kutesa A, Kagawa M, Mugyenyi G, et al. Periodontal conditions, low birth weight and preterm birth among postpartum mothers in two tertiary health facilities in Uganda. BMC Oral Health. 28 avr 2014; 14: 42. |
| [13] | Ibrahim HMEM, Mudawi AM, Ghandour IA. Oral health status, knowledge and practice among pregnant women attending Omdurman maternity hospital, Sudan. EMHJ-East Mediterr Health J. 2016; 22(11): 802-9. |
| [14] | Gupta S, Jain A, Mohan S, Bhaskar N, Walia PK. Comparative Evaluation of Oral Health Knowledge, Practices and Attitude of Pregnant and Non-Pregnant Women, and Their Awareness Regarding Adverse Pregnancy Outcomes. Clin Diagn Res JCDR. 2015; 9(11): ZC26-32. |
| [15] | Amit M, Hooja N, Mital P, Salvi A, Fatima A. Oral and dental health knowledge, attitude and practice among pregnant women. 2014; 2(9): 627-32. |
| [16] | Togoo RA, Al-Almai B, Al-Hamdi F, Huaylah SH, Althobati M, Alqarni S. Knowledge of Pregnant Women about Pregnancy Gingivitis and Children Oral Health. Eur J Dent. mai 2019; 13(02): 261-70. |
| [17] | Jafri Z, Bhardwaj A, Sawai M, Sultan N. Influence of Female Sex Hormones on Periodontium: A Case Series. J Nat Sci Biol Med. 2015; 6: 146-9. |
| [18] | Wu M, Chen SW, Jiang SY. Relationship between Gingival Inflammation and Pregnancy. Mediat Inflamm. 2015; 623427. |
| [19] | Figueiredo MGOP, Takita SY, Dourado BMR, Mendes HDS, Terakado EO, Nunes HRDC, et al. Periodon- tal Disease: Repercussions in Pregnant Woman and Newborn Health—A Cohort Study. PLoS ONE. 2019; 14. |
| [20] | Mealey BL, Moritz AJ. Hormonal influences: effects of diabetes mellitus and endogenous female sex steroid hormones on the periodontium. Periodontol 2000. 2003; 32: 59-81. |
| [21] | Silva de Araujo Figueiredo C, Gonçalves Carvalho Rosalem C, Costa Cantanhede AL, Abreu Fonseca Thomaz ÉB, Fontoura Nogueira da Cruz MC. Systemic alterations and their oral manifestations in pregnant women. J Obstet Gynaecol Res. janv 2017; 43(1): 16-22. |
| [22] | Donos N. The periodontal pocket. Periodontol 2000. févr 2018; 76(1): 7-15. |
| [23] | Rainchuso L. Improving Oral Health Outcomes from Pregnancy through Infancy. American Dental Hygienists’ Association. 2013; 87(6): 330-5. |
| [24] | Mesa F, Pozo E, O’Valle F, Puertas A, Magan-Fernandez A, Rosel E, et al. Relationship between periodontal parameters and plasma cytokine profiles in pregnant woman with preterm birth or low birth weight. Clin Oral Invest. 1 mai 2016; 20(4): 669-74. |
| [25] | McLoughlin IJ, Hassanyeh F. Pica in a patient with anorexia nervosa. Br J Psy. 1990; |
| [26] | Rabinerson D, Krispin E, Gabbay-Benziv R. Dental care during pregnancy. Harefuah. 2018; 157(5): 330-4. |
| [27] | Fairburn CG, Stein A, Jones R. Eating habits and eating disorders during pregnancy. Psychosom Med. 1992; 54: 665-72. |
| [28] | Ndjoh J, Metogo Ntsama J, Mengong H, Etounou Akono T, Nsahlai C, Zainam M, et al. Connaissances des Femmes Enceintes sur leur Santé Bucco-Dentaire dans la Ville de Maroua. 2022; 23(6): 76-80. |
| [29] | Vivares-Builes AM, Rangel-Rincón LJ, Botero JE, Agudelo-Suárez AA. Gaps in Knowledge About the Association Between Maternal Periodontitis and Adverse Obstetric Outcomes: An Umbrella Review. J Evid Based Dent Pract. mars 2018; 18(1): 1-27. |
| [30] | Dave BH, Shah EB, Gaikwad RV, Shah SS. Association of preterm low-birth-weight infants and maternal periodontitis during pregnancy: An interventional study. J Indian Soc Pedod Prev Dent. 2021; 39(2): 183-8. |
| [31] | Petrini DM, Gürsoy DM, Gennai DS, Graziani F. Biological mechanisms between periodontal diseases and pregnancy complications: a systematic review and meta-analysis of epidemiological association between adverse pregnancy outcomes and periodontitis - an update of the review by Ide & Papapanou (2013). |
| [32] | Petit C, Benezech J, Davideau JL, Hamann V, Tuzin N, Huck O. Consideration of Oral Health and Periodontal Diseases During Pregnancy: Knowledge and Behaviour Among French Pregnant Women. Oral Health Prev Dent. 2021; 19(1): 33-42. |
| [33] | Llena, Nakdali, Sanz, Forner. Oral Health Knowledge and Related Factors among Pregnant Women Attending to a Primary Care Center in Spain. IJERPH. 11 déc 2019; 16(24): 5049. |
| [34] | Zimmermann H, Zimmermann N, Hagenfeld D, Veile A, Kim TS, Becher H. Is frequency of tooth brushing a risk factor for periodontitis? A systematic review and meta-analysis. Community Dent Oral Epidemiol. avr 2015; 43(2): 116-27. |
| [35] | Axelsson P, Nyström B, Lindhe J. The long-term effect of a plaque control program on tooth mortality, caries and periodontal disease in adults. Journal of Clinical Periodontology. 2004; 31(9): 749-57. |
| [36] | Lang NP, Cumming BR, Löe H. Toothbrushing frequency as it relates to plaque development and gingival health. J Periodontol. juill 1973; 44(7): 396-405. |
| [37] | Worthington HV, MacDonald L, Poklepovic Pericic T, Sambunjak D, Johnson TM, Imai P, et al. Home use of interdental cleaning devices, in addition to toothbrushing, for preventing and controlling periodontal diseases and dental caries. Cochrane Database Syst Rev. 10 avr 2019; 4(4): CD012018. |
| [38] | Adeniyi A, Agbaje O, Braimoh M, Ogunbanjo O, Modupe S, Olubunmi O. A Survey of the Oral Health Knowledge and Practices of Pregnant Women in a Nigerian Teaching Hospital. Afr J Reprod Health. 2011; 15(4): 14-9. |
| [39] | Tang Y, Zhu Y, Wang Y, He Y. A survey about knowledge, attitude, practice of oral health in pregnant women of one hospital in Shanghai municipality. Shanghai Kou Qiang Yi Xue. 2011; 20(5): 531-4. |
| [40] | George A, Johnson M, Blinkhorn A, Ajwani S, Bhole S, Yeo A, et al. The oral health status, practices and knowledge of pregnant women in south-western Sydney. Aust Dent J. 2013; 68(1): 26-33. |
| [41] | Liu P, Wen W, Yu KF, Gao X, Lo ECM, Wong MCM. Effectiveness of a family-centered behavioral and educational counselling approach to improve periodontal health of pregnant women: a randomized controlled trial. BMC Oral Health. 16 oct 2020; 20(1): 284. |
| [42] | Gharehghani MAM, Bayani A, Bayat AH, Hemmat M, Karimy M, Ahounbar E, et al. Poor oral health-related quality of life among pregnant women: A systematic review and meta-analysis. Int J Dent Hyg. févr 2021; 19(1): 39-49. |
APA Style
Wendkouni, G. J. V., Hama, D. A., Ladifatou, O., Dan, K. F., Desire, K. W. A., et al. (2024). Knowledge, Attitudes and Practices of Pregnant Women on Oral Health in the University Hospitals of Ouagadougou, Burkina Faso. Central African Journal of Public Health, 10(2), 116-129. https://doi.org/10.11648/j.cajph.20241002.17
ACS Style
Wendkouni, G. J. V.; Hama, D. A.; Ladifatou, O.; Dan, K. F.; Desire, K. W. A., et al. Knowledge, Attitudes and Practices of Pregnant Women on Oral Health in the University Hospitals of Ouagadougou, Burkina Faso. Cent. Afr. J. Public Health 2024, 10(2), 116-129. doi: 10.11648/j.cajph.20241002.17
AMA Style
Wendkouni GJV, Hama DA, Ladifatou O, Dan KF, Desire KWA, et al. Knowledge, Attitudes and Practices of Pregnant Women on Oral Health in the University Hospitals of Ouagadougou, Burkina Faso. Cent Afr J Public Health. 2024;10(2):116-129. doi: 10.11648/j.cajph.20241002.17
@article{10.11648/j.cajph.20241002.17,
author = {Gare Jocelyne Valerie Wendkouni and Diallo Abdoulaye Hama and Ouedraogo Ladifatou and Kientega Filwendé Dan and Kabore Wendpoulomde Aime Desire and Kanoute Aida},
title = {Knowledge, Attitudes and Practices of Pregnant Women on Oral Health in the University Hospitals of Ouagadougou, Burkina Faso
},
journal = {Central African Journal of Public Health},
volume = {10},
number = {2},
pages = {116-129},
doi = {10.11648/j.cajph.20241002.17},
url = {https://doi.org/10.11648/j.cajph.20241002.17},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cajph.20241002.17},
abstract = {Knowledge of the relationship between pregnancy and oral health is a public health issue. The aim of this study was to assess the knowledge, attitudes and practices of pregnant women regarding oral health in the University Hospital Centers (UHC) of Ouagadougou in 2023. This was a descriptive cross-sectional study from July to September 2023. Data were collected prospectively, and knowledge, attitude and practice scores were generated. A total of 400 pregnant women were included. The [25-34] age group was the most represented at 54%, and 56.3% of women were in their 3rd trimester of pregnancy. The majority had a secondary level school and didn’t have a treating dentist. More than half (51.2%) of the respondents had poor overall knowledge of the relationship between oral health and pregnancy, 76.3% had poor attitudes and 79.5% poor practices, resulting in a poor overall KAP level for their oral health (60.5%). There was a significant variation in KAP level according to level of education (p= 0.015) and according to the information received on oral health and its implications for pregnancy (p = 0.028). Pregnant women's knowledge, attitudes and practices regarding their oral health are inadequate. Most women were unaware of the potential consequences of oral health neglect on pregnancy and their unborn child. Efforts must be made to educate them about oral health, with a focus on prevention.
},
year = {2024}
}
TY - JOUR T1 - Knowledge, Attitudes and Practices of Pregnant Women on Oral Health in the University Hospitals of Ouagadougou, Burkina Faso AU - Gare Jocelyne Valerie Wendkouni AU - Diallo Abdoulaye Hama AU - Ouedraogo Ladifatou AU - Kientega Filwendé Dan AU - Kabore Wendpoulomde Aime Desire AU - Kanoute Aida Y1 - 2024/04/28 PY - 2024 N1 - https://doi.org/10.11648/j.cajph.20241002.17 DO - 10.11648/j.cajph.20241002.17 T2 - Central African Journal of Public Health JF - Central African Journal of Public Health JO - Central African Journal of Public Health SP - 116 EP - 129 PB - Science Publishing Group SN - 2575-5781 UR - https://doi.org/10.11648/j.cajph.20241002.17 AB - Knowledge of the relationship between pregnancy and oral health is a public health issue. The aim of this study was to assess the knowledge, attitudes and practices of pregnant women regarding oral health in the University Hospital Centers (UHC) of Ouagadougou in 2023. This was a descriptive cross-sectional study from July to September 2023. Data were collected prospectively, and knowledge, attitude and practice scores were generated. A total of 400 pregnant women were included. The [25-34] age group was the most represented at 54%, and 56.3% of women were in their 3rd trimester of pregnancy. The majority had a secondary level school and didn’t have a treating dentist. More than half (51.2%) of the respondents had poor overall knowledge of the relationship between oral health and pregnancy, 76.3% had poor attitudes and 79.5% poor practices, resulting in a poor overall KAP level for their oral health (60.5%). There was a significant variation in KAP level according to level of education (p= 0.015) and according to the information received on oral health and its implications for pregnancy (p = 0.028). Pregnant women's knowledge, attitudes and practices regarding their oral health are inadequate. Most women were unaware of the potential consequences of oral health neglect on pregnancy and their unborn child. Efforts must be made to educate them about oral health, with a focus on prevention. VL - 10 IS - 2 ER -
Department of Public Health, Joseph Ki Zerbo University, Ouagadougou, Burkina Faso; Department of Dental Surgery, Joseph Ki Zerbo University, Ouagadougou, Burkina Faso
Department of Public Health, Joseph Ki Zerbo University, Ouagadougou, Burkina Faso
Department of Public Health, Joseph Ki Zerbo University, Ouagadougou, Burkina Faso
Department of Public Health, Joseph Ki Zerbo University, Ouagadougou, Burkina Faso; Department of Dental Surgery, Joseph Ki Zerbo University, Ouagadougou, Burkina Faso
Department of Dental Surgery, Joseph Ki Zerbo University, Ouagadougou, Burkina Faso
Public Health and Preventive Medicine Service, Cheikh Anta Diop University, Dakar, Senegal
Information